Here is the answer, straight away: syphilis is curable at every single stage. The first-line cure is benzathine penicillin G by injection — a single 2.4-million-unit dose clears primary, secondary and early-latent syphilis, per the CDC 2021 and WHO STI treatment guidelines. Later or unknown-duration syphilis takes three such injections, a week apart. One bacterium, one antibiotic, a complete cure.
As a practising andrologist in Chennai, I see the same fear every week: a man gets a reactive VDRL report, reads the word “incurable” attached to old descriptions of tertiary syphilis, and assumes his life is over. Let me settle that now. The man who walks in with a fresh reactive report almost always walks out cured after a single injection. The treatment is decades old, it is cheap, and it works. The rest of this article is the detail behind that — what syphilis is, how I test for it, and how I cure it.
Syphilis treatment in Chennai is short and curable. The CDC 2021 first-line cure is a single injection of benzathine penicillin G 2.4 million units for early syphilis (three weekly injections for late or unknown-duration disease). At Dr Shah’s Clinic in T. Nagar we confirm it with a VDRL/RPR and TPHA blood test and start treatment the same day — for you and your partner. Penicillin allergy is not a dead end: oral doxycycline is the standard alternative.
📍 No 21, Sree Kalki Apartments, Ground Floor, Bazullah Road, T-Nagar, Chennai 600017
📞 +91 97907 83856 · 🕘 Mon–Sat, 9:00 AM–6:00 PM · ⭐ 4.7 (800+ reviews)
Areas we serve in Chennai: T. Nagar, Anna Nagar, Velachery, Nungambakkam, Adyar, Tambaram, Chromepet, Porur and OMR — confidential STI testing and same-day treatment.
Quick Facts
- Syphilis is curable at every stage — penicillin G, given by injection, is the preferred drug for all stages (per CDC 2021).
- Early syphilis = one injection. A single dose of benzathine penicillin G 2.4 million units IM cures primary, secondary and early-latent syphilis.
- It is making a comeback. US syphilis crossed 209,000 cases in 2023 — a roughly 30-fold rise since 2000–2001 — so a reactive test today is far from rare (Treger, 2025).
- Penicillin allergy is not a dead end. Oral doxycycline 100 mg twice daily for 14 days is the standard alternative, and in a real-world HIV cohort it matched penicillin for cure (Nanoudis, 2024).
- Cure is tracked by a falling titre. A four-fold fall in your VDRL/RPR (say 1:32 to 1:8) confirms the cure is working (Workowski, 2021).
Everything that matters, in 60 seconds
The essentials an andrologist wants every man to know — what it is, what it does, and why it is completely curable when caught.
How it spreads
Direct contact with a syphilis sore during vaginal, anal or oral sex — including kissing when a sore is on the lip or mouth — and from mother to baby in pregnancy. Not from toilet seats or shared food.
The first sign
A single, firm, painless ulcer (a chancre) at the site of contact, about three weeks after exposure. Because it does not hurt and heals on its own, most men ignore it.
Why silence is the danger
The sore heals and a rash fades, so the infection looks gone. It is not — it goes latent and can surface years later in the heart, brain and nerves. Only a blood test finds it.
How it is diagnosed
Two blood tests together: VDRL/RPR (a titre that tracks activity) and TPHA/TPPA (confirms exposure, stays positive for life). A lumbar puncture is reserved for nerve or eye involvement.
The cure
Benzathine penicillin G by injection — one dose for early syphilis, three weekly doses for late disease (CDC 2021). Doxycycline is the oral alternative if you are penicillin-allergic.
Proof it worked
We repeat the VDRL/RPR at 6 and 12 months and watch the titre fall four-fold. A titre that sticks low (serofast) is not failure; a titre that climbs points to a new infection.
Syphilis treatment in Chennai: the penicillin cure, by stage
I will give you the whole protocol up front, because that is what you came for. Syphilis is caused by a single bacterium, Treponema pallidum, and that organism has never developed resistance to penicillin. Penicillin G, given by injection, remains the preferred treatment for patients in every stage (Workowski, 2021). The only thing that changes with stage is how many doses you need and which form of penicillin.
| Stage | First-line treatment | If penicillin-allergic |
|---|---|---|
| Primary, secondary or early-latent (under 1 year) | Benzathine penicillin G 2.4 million units IM, single dose | Doxycycline 100 mg twice daily for 14 days |
| Late-latent or unknown duration | Benzathine penicillin G 2.4 million units IM weekly × 3 (7.2 million units total) | Doxycycline 100 mg twice daily for 28 days |
| Neurosyphilis / ocular / otic | Aqueous crystalline penicillin G 18–24 million units/day IV for 10–14 days | Penicillin desensitisation preferred; IV ceftriaxone is an option |
| Pregnancy | Benzathine penicillin G by stage (above) | No true alternative — desensitise and give penicillin |
What is the first-line treatment for syphilis?
The first-line treatment for syphilis is benzathine penicillin G, full stop. For early syphilis that is one 2.4-million-unit injection into the buttock; for late or unknown-duration disease it is three of those injections at weekly intervals (Workowski, 2021). It is the only treatment proven to work in pregnancy and in neurosyphilis, which is why we go to the trouble of desensitising allergic patients rather than simply substituting another drug. If you have caught this early, your entire treatment is a single visit.
What is syphilis?
Syphilis is a sexually transmitted infection caused by the spiral-shaped bacterium Treponema pallidum. It is a great mimic — it moves through the body in stages, and at each stage it can look like something else entirely, which is exactly why it earned the old nickname “the great imitator.” Left alone it can smoulder silently for years and then surface in the heart, the brain or the nerves. Treated, it is one of the most reliably curable infections we have.
The important context for 2026 is that syphilis is not a disease of the past. After being pushed to near-elimination around the year 2000, it has risen sharply again — over 209,000 US cases in 2023, with the steepest rises among women and newborns (Treger, 2025). I see the same trend in my own clinic. So if your report is reactive, you are not an oddity; you are part of a global resurgence, and the response is straightforward and well-rehearsed.
What are the symptoms of syphilis in men? (by stage)
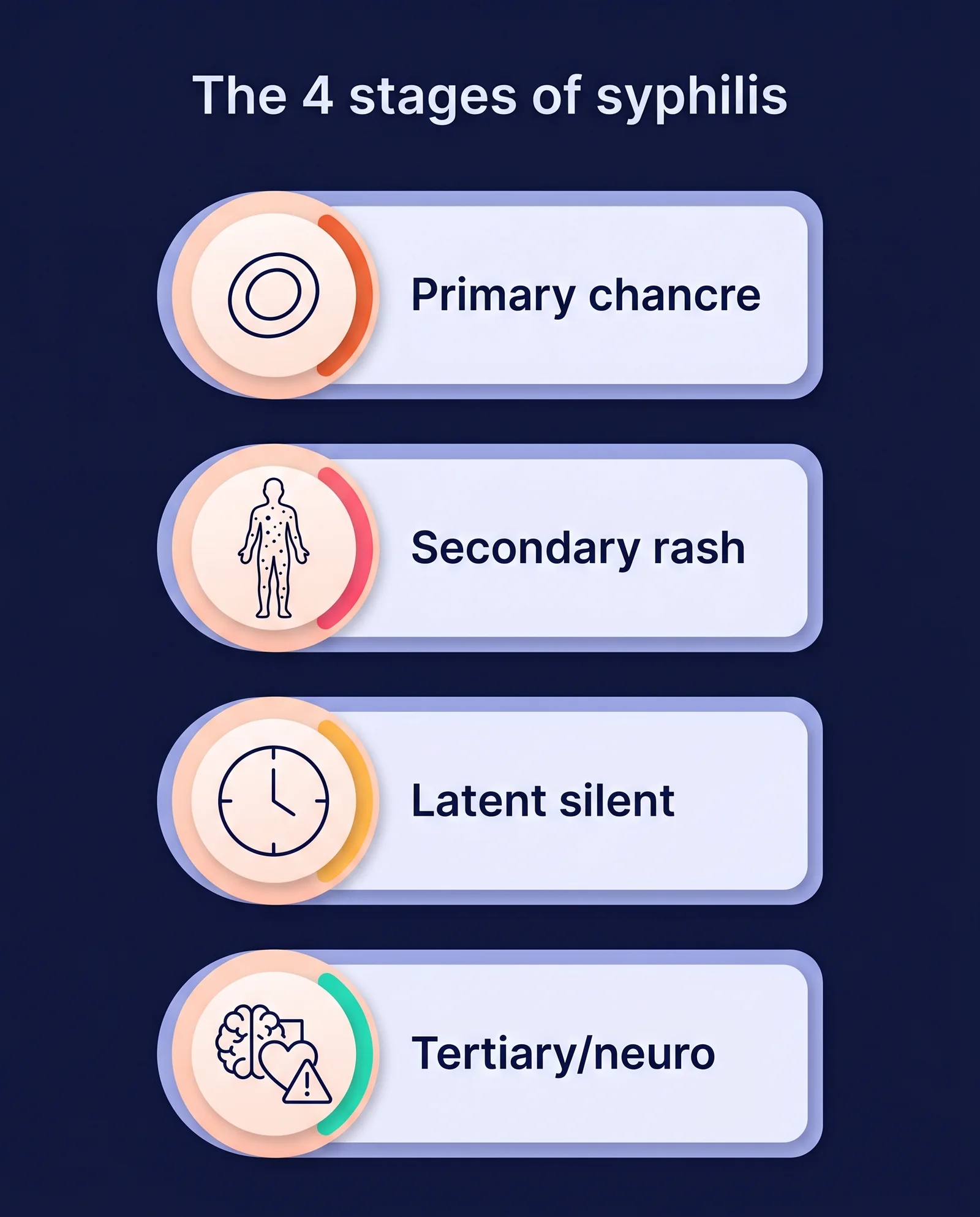
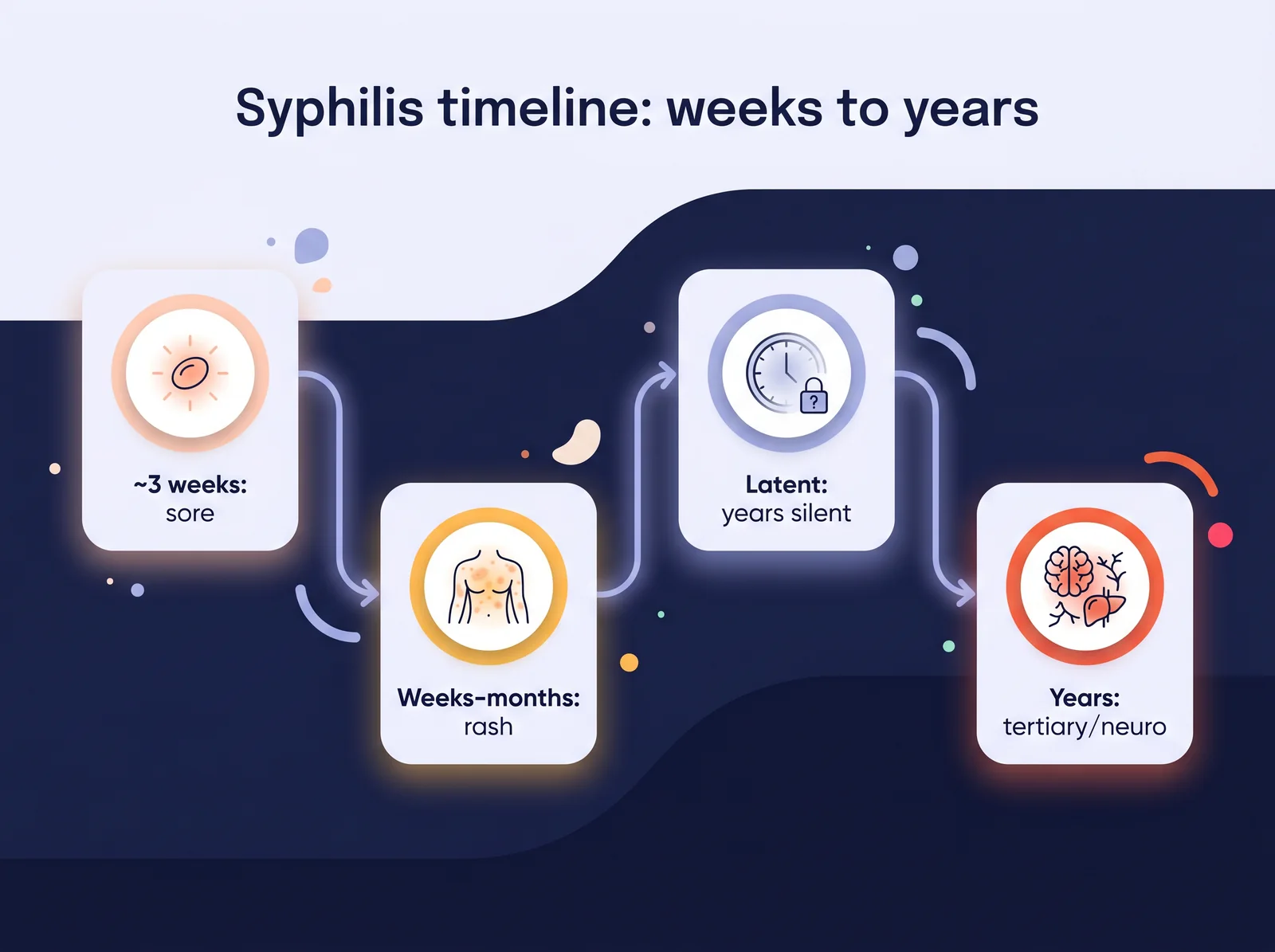
Syphilis announces itself differently depending on how long it has been with you. Here is what I look for, stage by stage.
Primary stage: the painless sore
The first sign is a chancre — a single, firm, round, usually painless ulcer at the spot where the bacterium entered: the penis, the anus, the lips or inside the mouth. Because it does not hurt, men ignore it, and because it heals on its own in three to six weeks, they assume the problem has gone. It has not. The sore healing is the infection moving inward, not leaving.
Secondary stage: the rash on palms and soles
Weeks to a few months later comes a body rash that classically involves the palms and soles — an unusual pattern that should always raise the question of syphilis. There may be flat warty patches around the genitals (condylomata lata), mouth ulcers, patchy hair loss, swollen glands and a flu-like malaise. This rash, too, fades by itself, which is precisely why so many cases slip into the latent stage undiagnosed.
Latent stage: the silent years
Now the disease goes quiet. No sore, no rash — but the bacterium is still there, detectable only on a blood test. Early-latent (under a year) and late-latent (over a year, or unknown duration) are treated slightly differently, which is why we always try to date your infection.
Tertiary and neurosyphilis: the serious end
In a minority left untreated for years, syphilis attacks the heart’s main vessel, forms destructive lumps called gummas, or invades the nervous system (neurosyphilis) — and that can show up as stroke-like episodes, dementia, or even a one-sided facial palsy mistaken for Bell’s palsy. This is the version people fear. It is also entirely preventable by treating the early disease in front of you today.
How do you get syphilis? (transmission and incubation)
Syphilis spreads through direct contact with a syphilis sore during vaginal, anal or oral sex. You can absolutely catch it from oral sex, and a chancre hidden inside the mouth or rectum means a partner can pass it on without either person seeing a thing. It also crosses the placenta from mother to baby — that is congenital syphilis. After exposure, the first sore typically appears in about three weeks, though it can range from 10 to 90 days. It does not spread through toilet seats, sharing food, or swimming pools. If you have had a recent exposure and an unexplained genital ulcer, do not wait for it to “declare itself” — get tested. The same logic applies to its frequent companions; I cover the overlap with gonorrhea symptoms and treatment and chlamydia testing and treatment on their own pages.
How is syphilis diagnosed? (VDRL, RPR and TPHA explained)
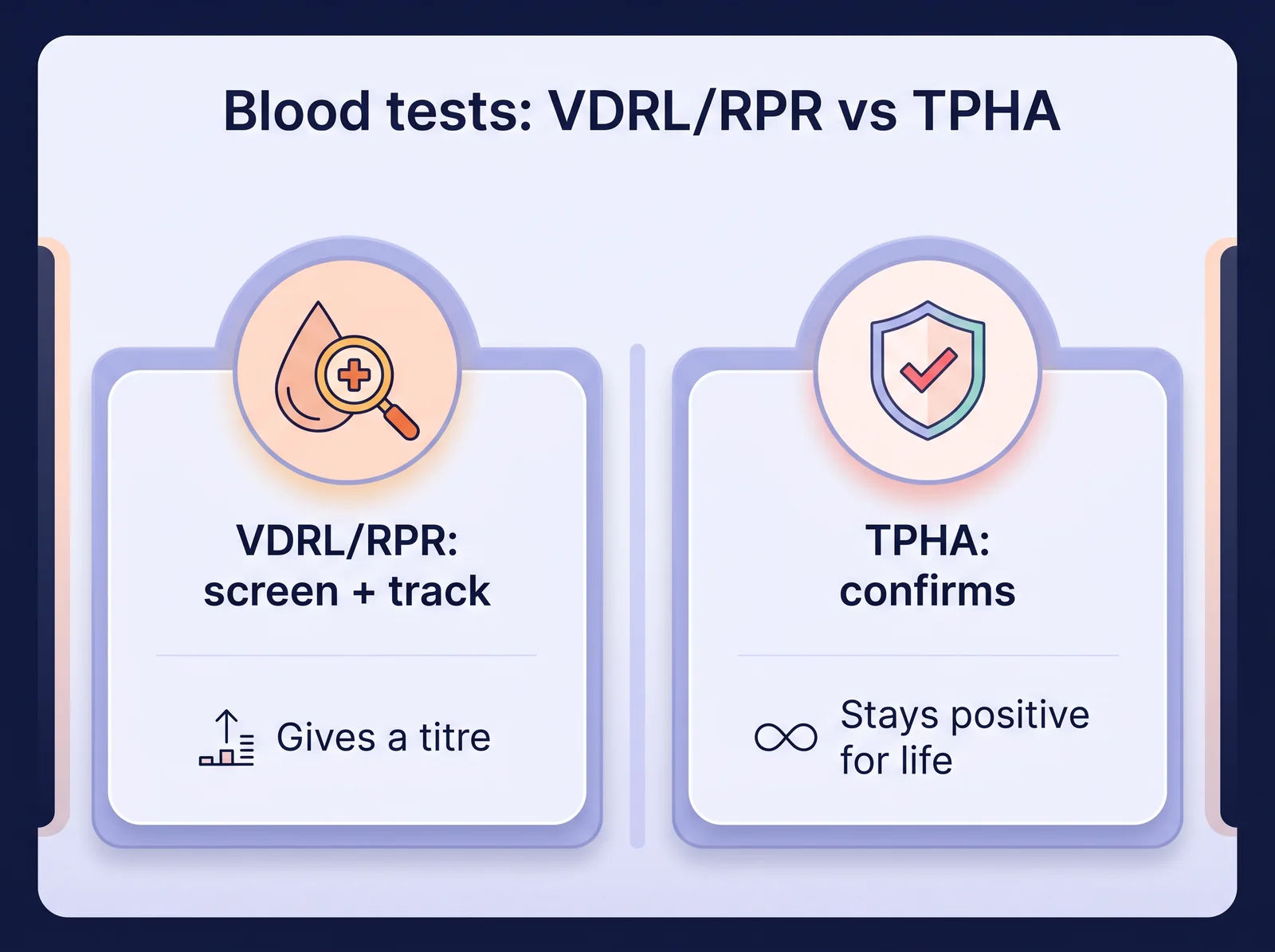
This is where most of my patients get confused, so let me make it simple. We use two kinds of blood test together, because neither alone tells the whole story (Treger, 2025).
Non-treponemal tests (VDRL / RPR)
VDRL and RPR measure the activity of the infection. They give a number — a titre — and that number rises with active disease and falls with successful treatment. These are the tests we screen and monitor with.
Treponemal tests (TPHA / TPPA / FTA-ABS)
TPHA, TPPA and FTA-ABS confirm that you have genuinely been exposed to Treponema pallidum. Once positive, they usually stay positive for life, even after a complete cure. So a positive TPHA years after treatment does not mean you are still infected — it is a scar, not an active wound.
What do the titres mean (1:2, 1:8, 1:32)?
The titre is how far we can dilute your blood and still see a reaction. A higher number means more active infection: 1:2 is low, 1:32 is high. We do not treat the number — we treat the person — but the titre is our scoreboard. After treatment we want to see it fall four-fold (two dilution steps), for example from 1:32 down to 1:8 (Workowski, 2021).
Serofast reaction
In some properly treated patients, the titre falls but then sticks at a low level — say 1:2 or 1:4 — and refuses to disappear. This is the serofast reaction, and it is one of the most over-treated misunderstandings in this whole field. In a 12-month Indian cohort, only about 63% reached full serological cure by one year, and a real share stayed serofast — without it meaning treatment had failed (Sethi, 2025). The newer immunological work shows this serofast state reflects a lingering immune over-activity rather than living bacteria, which is exactly why pumping in more antibiotics does not help (Kiolbasa, 2026). I tell these patients plainly: you are cured. The blood test is simply slow to normalise.
When is a lumbar puncture (CSF test) needed?
A spinal tap is not routine. I reserve it for patients with neurological or eye symptoms, very high titres that are not falling, or certain HIV-positive patients — to confirm or exclude neurosyphilis before deciding on IV treatment. Eye symptoms in particular matter: ocular syphilis often appears with no other signs at all, frequently alongside HIV, and it needs the same intravenous, neurosyphilis-level penicillin to save sight (Demirbas, 2026).
In my clinic, the hardest part of syphilis is never the treatment — it is the panic. The man with a reactive VDRL has usually already grieved his future by the time he reaches me, when the truth is that one injection will cure him. The two situations I actually have to manage are: the serofast patient who keeps demanding “one more course” because his titre will not hit zero — it does not need to — and the man who quietly skips telling his partner. I am gentle but firm on the second one: an untreated partner re-infects you within weeks, and then we are doing this all over again.
What if I am allergic to penicillin?
A genuine penicillin allergy is not a catastrophe. The main oral antibiotic used to treat syphilis when penicillin is out is doxycycline 100 mg twice daily — for 14 days in early syphilis, 28 days in late disease (Workowski, 2021). In a real-world HIV cohort, doxycycline matched benzathine penicillin for cure (Nanoudis, 2024). When an injectable alternative is preferred, ceftriaxone is the other choice — in a large neurosyphilis series it was used as an alternative to penicillin G, with a comparable Jarisch-Herxheimer reaction profile (Feng, 2026).
There are two exceptions where I will not accept a substitute: pregnancy and neurosyphilis. In those situations penicillin is the drug proven to protect mother, baby and brain — so if you are allergic, we desensitise you in a controlled setting and give the penicillin anyway. One caveat on the oral route: in confirmed early neurosyphilis, oral doxycycline has shown clinical and serological outcomes comparable to procaine penicillin (Girometti, 2021) — but that is a narrow specialist scenario, not a reason to skip injections in ordinary early syphilis. A penicillin allergy is a hurdle, never a wall.
The Jarisch-Herxheimer reaction (don’t panic after your injection)
A few hours after the first injection, some patients spike a fever, feel chills, get a headache, and watch their rash flare up briefly. Patients message me at midnight convinced the penicillin has poisoned them. It has not. This is the Jarisch-Herxheimer reaction — the immune system reacting to a flood of dying bacteria, not an allergy to the drug. It is self-limiting and settles within a day with rest, fluids and paracetamol (Ono, 2026). The best management is knowing it can happen, so I warn every patient before the first injection.
Follow-up: how do you know you’re cured?
Cure is not declared on the day of the injection — it is confirmed by a falling titre over the following months. I repeat the VDRL/RPR at 6 and 12 months (more often in HIV-positive patients) and look for that four-fold fall (Workowski, 2021). Most patients respond on schedule. Some take longer, and a minority stay serofast at a low titre — which, as above, is not failure and does not need re-treatment (Sethi, 2025; Kiolbasa, 2026). What would prompt me to act is a titre that climbs back up, which points to a new infection rather than a failed cure.
Syphilis, pregnancy and your baby (congenital syphilis)
This section matters more than any other, because syphilis in pregnancy is one of the few STIs that can harm a baby before birth. The good news is that treatment is straightforward and protective: benzathine penicillin G remains the WHO and CDC standard in pregnancy, and pharmacokinetic data confirm the weekly injection schedule keeps protective drug levels for weeks (Birru, 2026). In a ten-year hospital series, penicillin was given in 95% of pregnancies and produced an adequate four-fold antibody fall in 95% of treated mothers; the babies who still developed congenital syphilis were almost all born to women diagnosed late or treated inadequately (Cakir, 2026).
Two things I am firm about. First, penicillin is the only acceptable drug in pregnancy — an allergic mother must be desensitised, never switched to doxycycline. Second, a previous treated infection does not make a woman immune: in one large cohort, women with previously treated syphilis had markedly higher rates of reinfection and congenital syphilis than those never infected, which is exactly why every pregnancy needs fresh screening rather than a reliance on past treatment (Toppin, 2026). Treat early, screen again later in the pregnancy, and the baby is protected.
Syphilis rarely travels alone: HIV, chlamydia, gonorrhoea and herpes
A reactive syphilis test is a reason to test for everything else. Syphilis and HIV travel together so often that finding one demands looking for the other — in one high-risk cohort, nearly 1 in 10 people with HIV had syphilis, mostly the silent latent form, and standard penicillin still cured them effectively (Nanoudis, 2024). So when I treat syphilis, I also screen for HIV, hepatitis B and C, chlamydia testing and treatment, gonorrhoea and genital herpes treatment. If your HIV test comes back reactive, that too is a treatable, livable condition — I explain the pathway under HIV treatment in Chennai.
Complications of untreated syphilis
I include this not to frighten you but to explain why we treat even a silent, symptomless infection. Left untreated for years, syphilis can damage the aorta, form destructive gummas, and invade the brain and nerves as neurosyphilis — causing strokes, dementia, blindness and paralysis. In pregnancy it causes stillbirth and congenital disease. Every one of these belongs to the untreated disease. None of it happens to the man who takes his injection today. That is the entire point of this article.
Prevention and partner treatment
Prevention matters as much as the treatment itself. Consistent condom use lowers but does not fully eliminate risk, because a sore outside the covered area can still transmit. The non-negotiable step is partner treatment: anyone you have had sex with in the relevant window must be tested and treated, even if their tests are negative, because they may be incubating it (Workowski, 2021). I treat the couple, not just the patient — otherwise you simply re-infect each other. For broader screening and contact-tracing I point patients to our STD clinic in Chennai.
When should you see a doctor?
See me — or any STI clinician — if you have a painless genital, anal or oral ulcer; an unexplained rash on your palms and soles; a reactive VDRL/RPR or TPHA report; a known exposure to an infected partner; or you are pregnant and have not been screened. Sooner is always better, because early disease is a one-injection cure. If you are unsure what your numbers mean, bring the report in — I have seen men treated for the wrong stage, or terrified by a “positive TPHA” that was simply an old scar. If your worry is more about a cloudy discharge or pus cells in semen than an ulcer, that is a different conversation I am happy to have too, and you can also consult a sexologist in Chennai directly.

Private 1-on-1 consultation
Got a reactive VDRL report? One injection usually settles it — get it read properly.
Syphilis is curable at every stage, and the cure is tracked in numbers you can see fall. Confidential VDRL/TPHA testing and same-day penicillin treatment in Chennai.
Book a Confidential Consultation
Have your VDRL report read properly
A titre is easy to misread. Talk to Dr Shah, get the right number of injections, and watch the number fall.
Free guide · no spam · unsubscribe anytime.
Frequently asked questions about syphilis
Is syphilis curable?
Yes — syphilis is completely curable at every stage with the right antibiotic. Penicillin G clears the infection; the only difference between stages is the number of doses (Workowski, 2021). Caught early, it is a single injection.
What is the first-line treatment for syphilis?
Benzathine penicillin G 2.4 million units by intramuscular injection — one dose for early syphilis, three weekly doses for late or unknown-duration disease (Workowski, 2021). It is the preferred drug at every stage.
What is the first sign of syphilis in men?
A single, firm, painless ulcer (a chancre) at the site of contact — penis, anus, mouth or lips — appearing about three weeks after exposure. Because it does not hurt and heals on its own, it is easily missed.
How long after exposure do syphilis symptoms appear?
The first sore usually appears around 21 days after exposure, with a range of 10 to 90 days. The secondary rash follows weeks to months later.
Does the syphilis sore hurt?
Usually not. The classic chancre is painless, which is exactly why it gets ignored. A painful ulcer is more often herpes — but only testing tells them apart for certain.
What does the syphilis rash look like?
A reddish-brown rash that characteristically involves the palms and soles, often with flat genital patches, mouth sores and swollen glands. It typically does not itch and fades by itself even without treatment.
What is the difference between VDRL, RPR and TPHA?
VDRL and RPR measure disease activity and give a titre we use to screen and monitor. TPHA (and TPPA/FTA-ABS) confirm exposure and stay positive for life. We use one of each together (Treger, 2025).
Will my VDRL or TPHA become negative after treatment?
Your VDRL/RPR titre should fall, often to negative. Your TPHA usually stays positive for life — that is a scar of past infection, not a sign you are still infected. A small group stay serofast at a low VDRL titre, which is not treatment failure (Sethi, 2025).
What if I am allergic to penicillin?
Oral doxycycline 100 mg twice daily (14 days early, 28 days late) is the standard alternative, and in a real-world HIV cohort it matched benzathine penicillin for cure (Nanoudis, 2024). Where an injectable is preferred, ceftriaxone is the other option. The exceptions are pregnancy and neurosyphilis, where we desensitise you and give penicillin instead.
Can you get syphilis from kissing or oral sex?
Yes. A syphilis sore inside the mouth or on the lips can transmit through kissing or oral sex. The bacterium spreads by direct contact with a sore, not only through penetrative sex.
Do I need to tell and treat my partner?
Yes — without exception. Every recent partner must be tested and treated even if their own test is negative, because they may be incubating it. Skipping this is the commonest reason people get re-infected (Workowski, 2021).
References
- Centers for Disease Control and Prevention. Syphilis — STI Treatment Guidelines, 2021. cdc.gov/std/treatment-guidelines/syphilis.htm
- World Health Organization. Syphilis — fact sheet. who.int
- NHS. Syphilis. nhs.uk/conditions/syphilis
- Workowski KA, Bachmann LH, Chan PA, et al. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep. PMID 34292926
- Treger RS, et al. Advances in Syphilis Diagnostics to Address the 21st-Century Epidemic. Clin Chem. 2025. PMID 40510004
- Sethi S, et al. Predictors of serological cure and serofast stage after treatment in patients with syphilis: a retrospective study from India. Indian J Sex Transm Dis AIDS. 2025. PMID 41425034
- Kiolbasa M, et al. Serofast Syphilis Is Associated with Phospholipid-Dependent Coagulation Abnormalities and B-Cell Activation Following Treatment. Int J Mol Sci. 2026. PMID 42278482
- Ono T, et al. Incidence of Jarisch-Herxheimer Reaction After Syphilis Treatment and the Role of Awareness Effect. J Chin Med Assoc. 2026. PMID 42312658
- Girometti N, et al. Clinical and serological outcomes in patients treated with oral doxycycline for early neurosyphilis. J Antimicrob Chemother. 2021. PMID 33783506
- Birru E, et al. Pharmacokinetics of a three-dose regimen of intramuscular benzathine penicillin G in pregnant women with syphilis. J Antimicrob Chemother. 2026. PMID 42046912
- Toppin PJ, et al. History of Treated Syphilis Before Pregnancy and Risk of Congenital Syphilis. Obstet Gynecol. 2026. PMID 42096714
- Nanoudis S, et al. Prevalence and Treatment Outcomes of Syphilis among People with HIV Engaging in High-Risk Sexual Behavior: Real World Data from Northern Greece, 2019–2022. Microorganisms. 2024. PMID 39065024
- Feng X, et al. Jarisch-Herxheimer reaction as a complication of penicillin G and ceftriaxone treatment in neurosyphilis. BMC Infect Dis. 2026. PMID 41593451
- Demirbas ND, et al. Ocular syphilis: clinical characteristics, HIV status, and outcomes in a 10-year case series from Türkiye. Int J STD AIDS. 2026. PMID 41774527
- Cakir U, et al. Epidemiological and clinical characteristics of gestational and congenital syphilis in Hungary. Int J STD AIDS. 2026. PMID 41974120
This article is for education and does not replace an in-person consultation. If you have a reactive VDRL report or a possible syphilis exposure, get tested. Call +919790783856 to book a confidential appointment with Dr Shah Dupesh in Chennai.