
A quick, honest answer from Dr Shah Dupesh, MBBS — consultant Andrologist & Sexologist, Chennai. Last updated and medically reviewed July 2026, against current AUA and EAU guidance.
Is a curved penis normal? For most men, yes — almost always. Many men have some natural bend, and a curve in the commonly cited 5-to-30-degree range, in any direction — up, down, left or right — needs no treatment at all if it is painless, stable, and does not get in the way of sex. In one large population study, roughly 1 in 5 men (about 19%) reported a visible curve, and most were mild (Chung, 2018). A curve only becomes a medical problem — most often a condition called Peyronie’s disease — when it is greater than about 30 degrees, painful, newly changing, or comes with a hard lump you can feel.
So if you have gazed down and noticed your penis leans one way, take a breath. In my clinic, this is one of the single most common worries men bring me, and the great majority walk out reassured rather than treated. This guide tells you exactly where the line is — what is normal, how to measure it honestly, when to see a specialist, and every treatment that genuinely works if you do cross that line.
If you only read one thing here, read this – the essentials at a glance, before we go deeper.
Curved penis at a glance
A curve is common. About 1 in 5 men (19%) report a visible curve, and most are mild – a straight penis is still the norm, but a slight bend is completely normal.
Roughly 5-30° is the normal zone. If it is painless, stable and sex works, no treatment is needed – a clinical threshold, not a defect.
Over ~30°, painful, a lump, or newly changing = get assessed. This is the pattern of Peyronie’s disease.
Peyronie’s is not rare – roughly 0.5%-13% of men, most often in the 50s-60s but sometimes earlier.
It rarely straightens on its own. An early, untreated Peyronie’s curve improves in only ~12% and worsens in nearly half.
Real treatments exist – traction, collagenase injections and surgery all straighten curves. Oral cures and exercises do not.
Is a curved penis normal?
Let me be direct, because this is the question that keeps men awake at night: yes, in the overwhelming majority of cases, a curved penis is completely normal. The penis is not a straight steel rod; it is a paired erectile organ, and small differences in how the two chambers (the corpora cavernosa) and their surrounding sheath (the tunica albuginea) fill and stretch will tip an erection slightly one way. That is anatomy, not disease.
When Chung and colleagues surveyed nearly 1,800 men aged 35–75, about 19% reported some curve, and only around a third of those described it as 30 degrees or more (Chung, 2018). In other words, a mild bend is one of the most ordinary things about the male body.
What counts as “normal”?
There is an important nuance most websites get wrong, so I want you to hear it from a clinician: no measurement study has ever defined a precise “normal number of degrees.” The commonly quoted “up to about 30 degrees is fine” is a clinical and guideline threshold — the point below which urologists agree a curve almost never needs fixing — not a statistical average. What actually matters is the trio I use in clinic: is it painless, is it stable (not changing month to month), and does sex work comfortably for you and your partner? If the answer to all three is yes, the exact number barely matters — the same reassurance I give men worried about penis size.
Which way can it curve — up, down, left, or “C-shaped”?
Any direction is possible and can be normal. An upward curve is the most talked-about; downward, sideways (left or right), and even a gentle C-shape are all seen. A slight upward tilt is so common that many partners never register it as unusual at all.
Kya ling ka tedha hona normal hai? (Is a bent penis normal?)
Haan — thoda tedhapan bilkul normal hai. In my Chennai practice a great many men ask “ling kitna teda hona chahiye?” (how much bend is acceptable) and “ling tedha kyon hota hai?” (why does it bend at all). The honest answers: a curve is usually either present from birth (congenital) or develops later from an injury or Peyronie’s; and a mild, painless, stable curve needs no ilaj (treatment) at all. It is only when the bend is severe, painful, or suddenly increasing that you should see an andrologist.
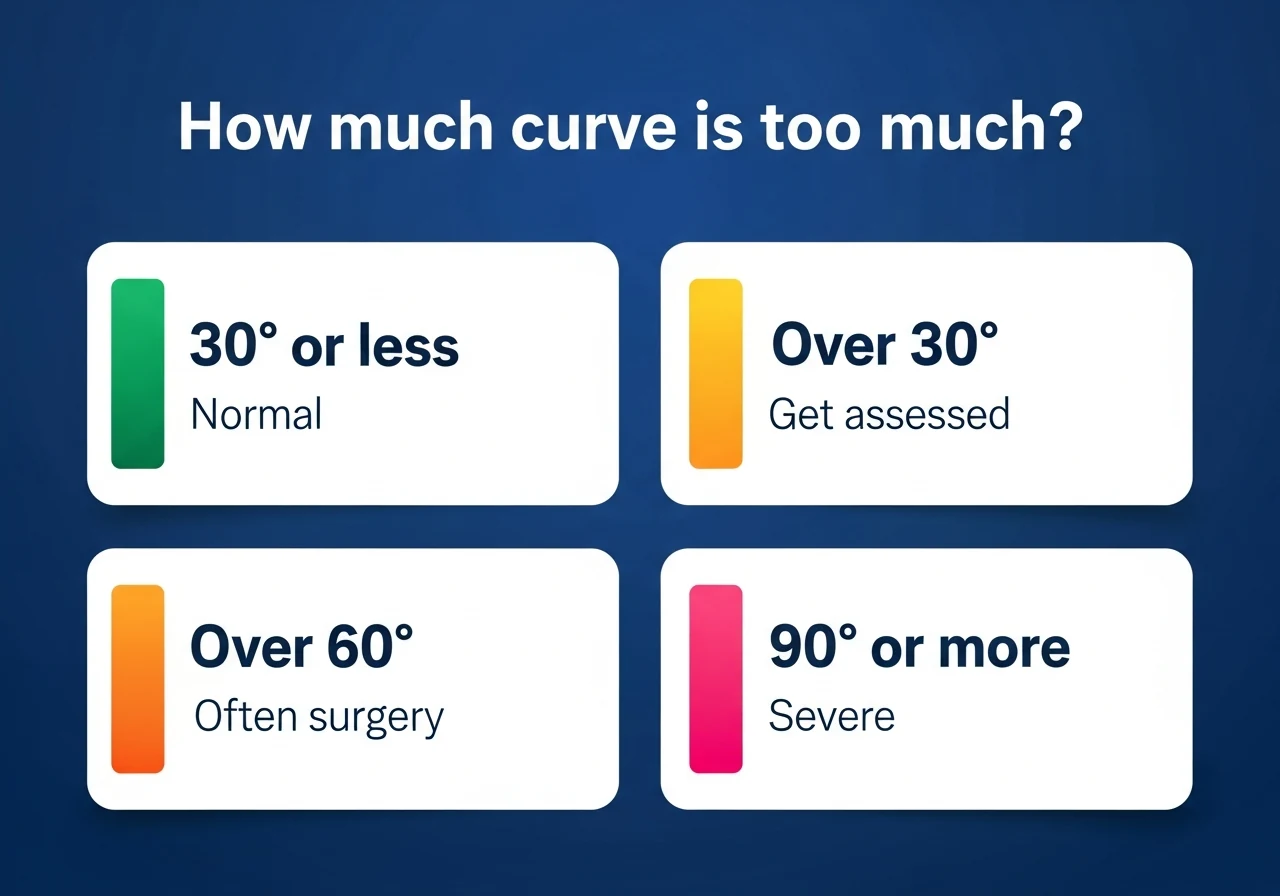
How much curve is too much? The degree framework
Here is the single most useful thing in this article — a clear ladder that tells you where your curve sits. This reconciles the numbers you will see quoted everywhere into one honest framework, built from the AUA and EAU guidelines (Nehra, 2015; Hatzimouratidis, 2012).
| Curve | What it usually means | What to do |
|---|---|---|
| ~5-30° | Normal variation, if painless, stable and sex is fine | Reassurance – no treatment needed |
| Over ~30° | Worth assessing; may be early/mild Peyronie’s; the treatment threshold | See an andrologist; medical options open here |
| Over ~60° | Significant curve; grafting-type surgery is typical, though a stable 60-90° curve with good erections may try collagenase or traction first | Specialist assessment |
| ≥90° (severe) | Frequently prevents intercourse | Strong surgical candidate |
One important caveat: these bands describe an acquired curve (Peyronie’s disease). A stable, lifelong curve of the same number of degrees is usually congenital — not a disease — and is judged on whether it interferes with sex, not on degrees alone.
Two caveats I always add. First, degrees are not the whole story — a 25-degree curve with pain and a growing plaque needs attention more urgently than a stable 35-degree curve that has been there for years. Second, the injectable drug collagenase is used only for stable curves in the 30–90 degree range with intact erections (Nehra, 2015), a useful real-world marker of the “treatable but not yet extreme” middle band (Gelbard, 2013).
When to see a doctor — the red flags
See an andrologist if you notice any of these:
– A new or suddenly worsening curve
– Pain on erection, or a painful erection that is also softer than before
– A hard lump or ridge (plaque) you can feel along the shaft
– Narrowing, an indentation, or an “hourglass” look during erection
– A curve over 30 degrees, or any curve that prevents comfortable sex
– Erectile dysfunction appearing alongside the curve
– Significant anxiety or relationship strain because of it
How to measure a curved penis (at home)
Men constantly under- or over-estimate their own curve, usually by eyeballing a soft or half-hard penis. Do it properly:
- Measure at full erection, not flaccid — the curve only shows truthfully at full rigidity.
- Photograph from three angles — top-down, and both sides — against a plain background, ideally with a straight reference edge (a ruler or the edge of a book) in frame.
- Estimate the angle of deviation from the straight line of the shaft; a printed or on-screen protractor/goniometer over the photo gives a far better number than guessing.
- Confirm in clinic if it matters — self-measurement is only a screen. We measure the true curve after an intracavernosal injection produces a full, standardised erection (the gold standard), because that is what surgeons plan around.
What causes penile curvature?
Broadly, a curve is either something you were born with (congenital) or something you developed later (acquired) — and telling them apart is the first job in clinic.
Congenital penile curvature (chordee)
Some men have had a curve for as long as they can remember. This congenital curvature — often called chordee without hypospadias when the urine opening is in the normal place — comes from the two sides of the tunica albuginea growing at slightly different rates. It is reported in a few percent of boys and men without hypospadias, with a wide range across studies, and the ventral (downward) direction is the classic pattern (Montag & Palmer, 2011; Menon, 2016). The key facts: a congenital curve is stable, painless, and has no plaque — and it does not straighten by itself. If it is mild it needs nothing; if it interferes with sex it is corrected surgically (usually a plication procedure).
Acquired curvature — Peyronie’s disease and injury
A curve that appears in adulthood, changes over weeks to months, or comes with pain or a lump is acquired, and the commonest cause by far is Peyronie’s disease (covered in detail below). The underlying mechanism is thought to be repetitive micro-trauma to the tunica albuginea — the buckling stress an erect penis takes during intercourse — triggering abnormal, scar-like healing in men who are predisposed (Sharma, 2020).
Erection angle and age
One reassuring point that gets missed: erection angle tends to decrease gradually with age — an erection that once stood high may sit more horizontal in your 50s and 60s. This is a change in angle, not a curve or a disease. That said, a new or rapid change in angle or shape is still worth getting checked.
A short frenulum (frenulum breve) — a fixable cause of downward tilt
Not every downward bend comes from the tunica or from Peyronie’s. In some men a short, tight frenulum — the small band of skin under the head of the penis, a condition called frenulum breve — tethers the glans downward, so the tip pulls down on erection, sometimes with tension or a small tear during sex. This is a mechanical, skin-level cause, quite different from a plaque or a congenital tunica curve — and it is easily corrected (see the treatment section).
Peyronie’s disease — the main medical cause
What is it?
Peyronie’s disease is the formation of a fibrous scar (plaque) in the tunica albuginea, the tough sheath around the erectile chambers. Because the plaque cannot stretch like normal tissue, the penis bends toward it during erection. It runs in two phases: an acute (active) phase — pain and an evolving curve, lasting weeks up to about a year — and a chronic (stable) phase, where the pain settles and the curve becomes fixed.
Symptoms
The three most common presentations are pain on erection, an abnormal upward or sideways tilt, and erectile dysfunction. The fuller picture I see in clinic:
– Pain on erection (typical of the active phase)
– An abnormal bend or tilt that is new or worsening
– A palpable hard lump or ridge along the shaft
– Penile shortening, narrowing, indentation, or an hourglass deformity
– Erectile dysfunction — very common alongside Peyronie’s
– Painful intercourse for you or your partner
In one large series, erectile dysfunction was present in over half (54%) of men with Peyronie’s, and two-thirds carried at least one vascular risk factor such as diabetes or high cholesterol (Kadioglu, 2002). There is also a well-known link with Dupuytren’s contracture of the hand, which coexists in about 1 in 5 Peyronie’s patients (Nugteren, 2011).
How common is it, and who gets it?
More common than most men think. Population surveys put it at 3.2% (Schwarzer, 2001) and anywhere from 0.5% up to about 13% depending on whether you count formal diagnoses or symptoms (DiBenedetti, 2011); when doctors actually examine men, palpable plaques turn up in nearly 9% (Mulhall, 2004). It is most often diagnosed in men in their 50s and 60s — though it can appear from the 40s, and occasionally earlier — and is almost certainly under-reported because men are too embarrassed to raise it (Stuntz, 2016).
Does it get better on its own?
Rarely — and this is the fact that changes decisions. In a prospective natural-history study of men with recent, untreated Peyronie’s, over about 18 months the curve improved in only 12%, stayed the same in 40%, and worsened in 48%; the good news was that penile pain resolved in nearly 90% (Mulhall, 2006). Earlier work found only about 13% of men perceive spontaneous improvement (Gelbard, 1990). So waiting rarely straightens things — but waiting for the pain to settle and the curve to stabilise is exactly what we do before offering surgery.
How is it diagnosed?
Diagnosis is clinical and straightforward: feeling the plaque on examination (palpation), combined with a penile duplex Doppler ultrasound to map the plaque and check blood flow, and an objective angle measurement taken after an injection-induced erection. No blood test diagnoses Peyronie’s.
How to straighten a bent or curved penis (the treatment ladder)
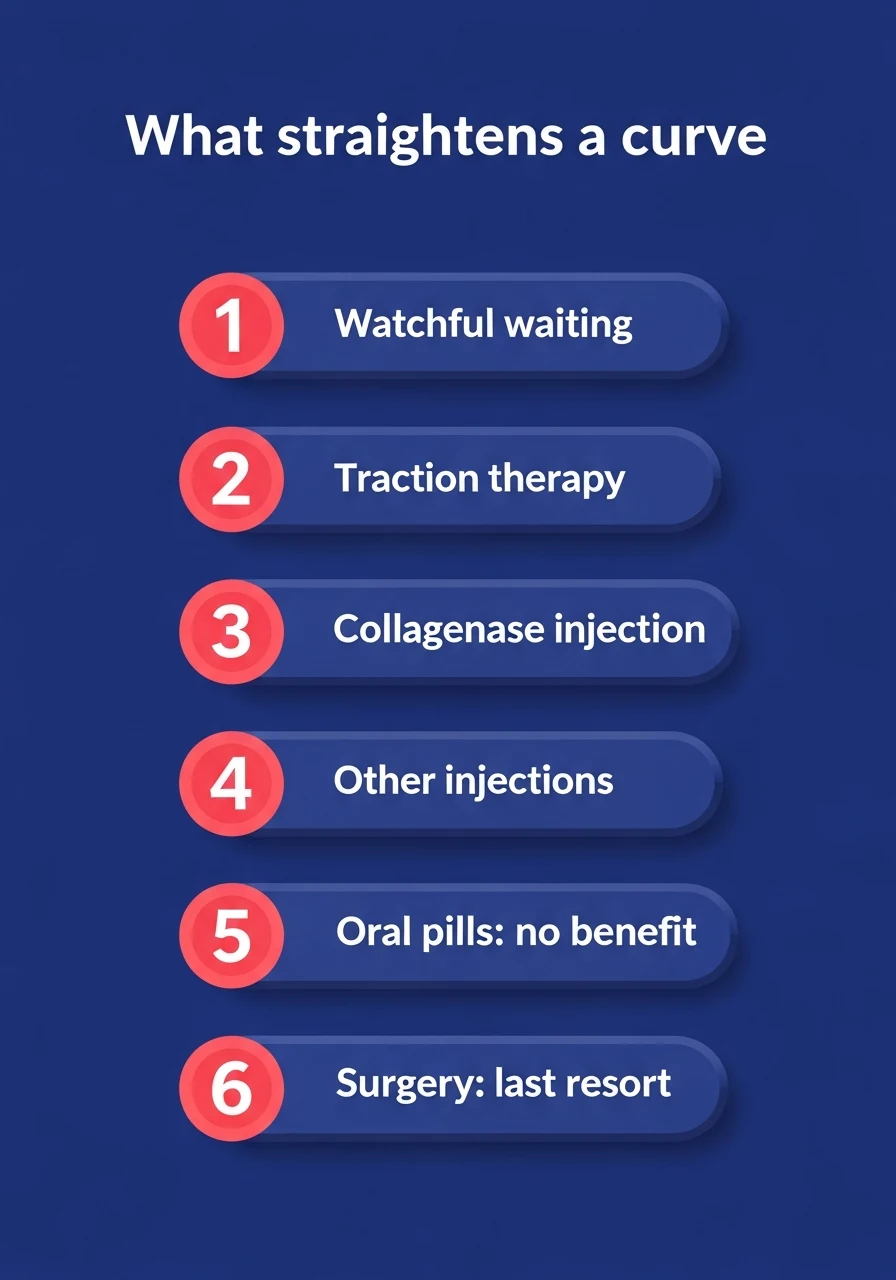
What actually straightens a curve
Watchful waiting – for a stable, painless curve that does not affect sex.
Traction therapy – a daily device; ~12° of correction in trials.
Collagenase (Xiaflex) – the only FDA-approved drug, for stable 30-90° curves.
Other injections – interferon (modest); verapamil (weak evidence).
Oral pills – do NOT straighten a curve. Vitamin E is not recommended.
Surgery – a last resort (real ED risk); reserved for severe, stable curves that prevent sex.
If you genuinely need treatment, here is the full ladder — from doing nothing, up to surgery — with what the evidence actually shows. I have deliberately included what does not work, because the internet is full of expensive nonsense.
1. Watchful waiting
For a mild, stable, painless curve that does not affect sex — congenital or Peyronie’s — the right treatment is often none. Reassurance and review is a legitimate, guideline-backed choice. But this applies only to a stable, painless curve: a new, painful, or actively worsening curve should be assessed promptly, not simply watched.
2. Penile traction therapy
A mechanical traction device worn daily can genuinely reduce curvature. In a randomised trial of the RestoreX device, men gained about −11.7 degrees of correction versus +1.3 degrees in controls at three months, plus a small length gain, with only mild side-effects (Ziegelmann, 2019). It takes commitment (typically ~30 minutes, once or twice daily, over weeks) but it is non-invasive and evidence-based.
3. Injections into the plaque
- Collagenase (Xiaflex) is the only FDA-approved drug for Peyronie’s. In the pivotal IMPRESS trials it improved curvature by about 17 degrees (34%) versus 9 degrees (18%) for placebo (Gelbard, 2013). It is used for stable curves of 30–90 degrees with intact erections (Nehra, 2015) — specifically dorsal or lateral curves with a palpable, non-calcified plaque. Importantly, it is given only by a trained specialist, carries a small but real risk of penile fracture and bruising, and needs a defined recovery protocol (no sexual activity for about two weeks) between injection cycles.
- Interferon-α2b gives a modest but real improvement in curve, plaque and pain versus placebo (Hellstrom, 2006).
- Verapamil injections are widely used but rest on low-quality evidence (Rehman, 1998), so I frame them honestly as an option, not a proven fix.
4. Oral medicines — the honest truth
No oral tablet reliably straightens an established curve. POTABA may slow progression but does not straighten an existing bend (Weidner, 2005), and the AUA guideline specifically recommends against oral vitamin E and POTABA for curvature (Nehra, 2015). Vitamin E, in particular, does not work — please do not spend money on it. Oral tadalafil or pentoxifylline are sometimes used adjunctively, but not as a stand-alone straightening cure.
5. Surgery
For a stable, significant curve, surgery is the most reliable straightener:
– Plication / Nesbit procedures (stitching or tucking the longer side) straighten the penis in the great majority of men — reported ranges run plication 58–100%, Nesbit 79–100%, commonly around 80–85% in practice — and are first-line for milder curves with good erections; the trade-off is some penile shortening, and roughly 15–20% report a complication such as shortening or a little residual curve (Mandava, 2013).
– Plaque incision/excision + grafting is reserved for severe or complex curves (over ~60°) and straightens in about 74–100%, but carries a higher risk of new erectile dysfunction (Mandava, 2013).
– A penile implant (prosthesis), often with straightening, is the answer when significant ED already coexists with the curve.
Crucially, guidelines say operate only once the disease is stable — pain-free and non-progressive for at least about 3 months (generally after the active phase, often ~6–12 months from onset) (Hatzimouratidis, 2012; Nehra, 2015). In my own practice I am deliberately cautious with straightening surgery because of that post-operative ED risk, and I reserve it for the rare severe, stable curve that genuinely prevents intercourse — non-surgical options handle the great majority.
A special case: frenuloplasty for a short-frenulum downward tilt
If a downward tilt is coming from a short frenulum (frenulum breve) rather than the tunica, the fix is quick and specific: a frenuloplasty releases the tethering band in about five minutes and reduces the downward angle. It does nothing for a Peyronie’s or congenital tunica curve, but for the right patient it is a simple, high-satisfaction solution — and one I reach for far more often than straightening surgery.
What about jelqing, “exercises,” and natural straightening?
There is no evidence that jelqing, stretching routines, or supplements straighten a curved penis, and aggressive manual techniques — the same forceful habit that makes prone masturbation risky — can cause the very micro-trauma that may trigger Peyronie’s. Skip them.
Does a curved penis affect sex or fertility?

Does a curved penis affect fertility?
Fertility: no. A mild or normal curve does not reduce sperm quality or your ability to father a child. The only way any curve affects conception is mechanical — a severe curve that physically prevents comfortable vaginal penetration. Therefore, for the vast majority of men with an ordinary curve, this is simply not a fertility issue.
Does a curved penis affect sex?
Most mild curves cause no trouble at all. However, where a curve does get in the way, simply adopting different positions during intercourse usually lets a couple accommodate the bend comfortably — something I coach patients through routinely. Real difficulty tends to appear only with more pronounced curves; indeed, men with a curve report more trouble with intercourse and more distress than men without one (Menon, 2016) — which is exactly the situation treatment is designed to fix.
Do women prefer a curved penis?
There is no good evidence that a curve is preferred or disliked in general; instead, partner comfort depends far more on communication and severity than on a few degrees of bend. In short, a mild curve is not something to feel self-conscious about.
The psychological side — anxiety, self-image, relationships
I want to name this plainly because men rarely admit it: a curved penis, and Peyronie’s especially, can weigh heavily on mood, confidence and relationships. The distress is real and it is common — and it is treatable. If your curve is normal, understanding why it is normal usually lifts the worry entirely. If it is Peyronie’s, know that the physical and the emotional both respond to treatment, and that raising it with an andrologist is the first step, not the awkward one.
Can a curved penis be prevented, and what’s the outlook?
You cannot reliably prevent a curve. A congenital curve is set before birth, and Peyronie’s follows the kind of micro-injury that is largely unavoidable — though avoiding forceful bending during sex, and keeping conditions like diabetes well controlled, may lower the odds. The outlook is genuinely reassuring: a normal curve stays normal and needs nothing; and while Peyronie’s rarely straightens fully on its own, once it stabilises it responds well to traction, injections or surgery. The men who do best are the ones who get assessed early rather than suffering in silence.
Dr Shah’s notes (from my clinical observation)
In day-to-day practice, a large share of the men who come to me anxious about a “bent” penis have an entirely normal, mild curve — and the single most valuable thing I do is measure it honestly and reassure them. My rule of thumb in clinic: a curve that is painless, stable, and compatible with satisfying sex almost never needs treatment, whatever its exact degree. What genuinely earns a proper work-up is a change — a new bend, new pain, a lump you can feel, or a curve that is quietly getting worse. When those are present, I examine, scan with a Doppler, and stage the disease before we discuss anything invasive. And I tell every patient the same thing I have written here: the real treatments are traction, injections and surgery — the pills and “exercises” sold online are, at best, a waste of money.
Three things from my own practice I especially want you to hear. First, I have essentially never recommended straightening surgery for a bent penis — the post-surgical risk of erectile dysfunction is real, and in my hands traction, injections, frenuloplasty (where a short frenulum is the cause), and simple changes of position solve the vast majority of cases without it. Second, for a downward tilt caused by a short frenulum (frenulum breve), a five-minute frenuloplasty has given many of my patients a quick, lasting improvement. And third, for a bend that is otherwise harmless, I coach couples through positions that comfortably accommodate the curve — often that alone is all the “treatment” anyone needs.

Private 1-on-1 consultation
Not sure if your curve is normal? Let’s check it properly.
A short, private assessment tells you within one visit whether you are in the normal zone or whether Peyronie’s is developing – and what, if anything, to do.
Book a Confidential Consultation
When should you see an andrologist?
If your curve is new, painful, over about 30 degrees, coming with a lump, getting worse, or affecting your sex life or your peace of mind — that is worth a consultation. A short, private assessment with an experienced andrologist in Chennai — or, for sexual-health concerns, a sexologist in Chennai can tell you within one visit whether you are firmly in the normal zone or whether Peyronie’s is developing, and what (if anything) to do about it.
Frequently asked questions
Is it normal for my penis to curve when erect?
Yes. A slight curve is common; about 1 in 5 men report a visible one, and the great majority are mild and completely normal (Chung, 2018).
How many degrees of curve is too much?
As a rule of thumb, a curve up to about 30 degrees that is painless and stable is normal. Over 30 degrees, or any curve with pain, a lump, or that is changing or preventing sex, should be assessed.
Can a curved penis be straightened without surgery?
Sometimes. Penile traction devices and collagenase (Xiaflex) injections both reduce curvature with good evidence in Peyronie’s disease (Ziegelmann, 2019; Gelbard, 2013). Oral tablets and exercises do not straighten an established curve.
Does a curved penis go away on its own?
A congenital curve does not self-correct. A Peyronie’s curve improves on its own in only about 12–13% of men and often worsens if untreated, though the pain usually settles (Mulhall, 2006; Gelbard, 1990).
Is a curved penis bad for sex or fertility?
No for fertility — a mild curve does not affect sperm or conception. It only matters mechanically if a severe curve prevents intercourse. Most mild curves cause no sexual problems at all.
Why is my penis bent to one side?
A stable, lifelong sideways or C-shaped bend is usually congenital and normal. A new, changing, or painful sideways bend — especially with a lump — should be checked for Peyronie’s disease.
Ling ka tedhapan kaise theek karein? (How do I fix a bent penis?)
A mild, painless bend needs no treatment. If it is severe, painful or worsening, see an andrologist — real options are traction therapy, plaque injections, and surgery; oral “cures” do not work.
Can a short frenulum cause a downward-curved penis?
Yes. A short, tight frenulum (frenulum breve) can tether the head of the penis downward, causing a downward tilt on erection. Unlike a tunica or Peyronie’s curve, this is corrected with a simple, roughly five-minute frenuloplasty — one of the quickest fixes in this whole area.
Can I fix a curved penis with exercises or jelqing?
No. There is no evidence exercises or jelqing straighten a curve, and forceful techniques can injure the penis and potentially trigger Peyronie’s. Avoid them.
References
- Chung E, et al. Penile curvature in men: a population-based study. BJU Int. 2018. (PMID 30387224)
- Schwarzer U, et al. The prevalence of Peyronie’s disease: results of a large survey. BJU Int. 2001. (PMID 11890244)
- DiBenedetti DB, et al. A population-based study of Peyronie’s disease. Adv Urol. 2011. (PMID 22110491)
- Mulhall JP, et al. Subjective and objective analysis of the prevalence of Peyronie’s disease. J Urol. 2004. (PMID 15126819)
- Stuntz M, et al. The prevalence of Peyronie’s disease in the United States. PLoS One. 2016. (PMID 26907743)
- Mulhall JP, et al. Natural history of Peyronie’s disease. J Urol. 2006. (PMID 16697815)
- Gelbard MK, et al. The natural history of Peyronie’s disease. J Urol. 1990. (PMID 2231932)
- Kadioglu A, et al. A retrospective review of 307 men with Peyronie’s disease. J Urol. 2002. (PMID 12187226)
- Nugteren HM, et al. Peyronie’s disease and Dupuytren’s contracture. Int J Impot Res. 2011. (PMID 21633367)
- Sharma KL, et al. The etiology of Peyronie’s disease: a review. Sex Med Rev. 2020. (PMID 31540807)
- Gelbard M, et al. Collagenase clostridium histolyticum for Peyronie’s disease (IMPRESS I & II). J Urol. 2013. (PMID 23376148)
- Hellstrom WJG, et al. Intralesional interferon-α2b for Peyronie’s disease. J Urol. 2006. (PMID 16753449)
- Rehman J, et al. Intralesional verapamil for Peyronie’s disease. Urology. 1998. (PMID 9586617)
- Ziegelmann M, et al. Randomized trial of the RestoreX penile traction device. J Urol. 2019. (PMID 30916626)
- Weidner W, et al. Potassium para-aminobenzoate (POTABA) for Peyronie’s disease. Eur Urol. 2005. (PMID 15774254)
- Mandava SH, et al. Surgical outcomes for Peyronie’s disease. Arab J Urol. 2013. (PMID 26558094)
- Nehra A, et al. Peyronie’s Disease: AUA Guideline. J Urol. 2015. (PMID 26066402)
- Hatzimouratidis K, et al. EAU Guidelines on Penile Curvature. Eur Urol. 2012. (PMID 22658761)
- Montag S, Palmer LS. Abnormalities of penile curvature: chordee and penile torsion. ScientificWorldJournal. 2011. (PMID 21805016)
- Menon P, et al. Do adult men with untreated ventral penile curvature have adverse outcomes? J Pediatr Urol. 2016. (PMID 26776946)
A private, judgment-free space to talk through fertility and men’s sexual health. Walk in, or book ahead by phone.
📍No 21, Sree Kalki Apartments, Ground Floor, Bazullah Road, T-Nagar, Chennai 600017
Any suggestions. I’m 68, I’ve never had an issue, intel about 2 weeks ago. I noticed a significant bend close to the base of my penis. I’m rather concerned. I’ve had no engery . Should I see a doctor, or is this a part of aging?
Rodney could you please rule out peyronie’s disease?