
Yes — it can. Of all the worries men bring me about masturbation, this is the one where the answer is genuinely “yes.” An unusual or very intense masturbation style is a recognised — and, in my clinical experience, frequently overlooked — cause of delayed ejaculation in otherwise healthy young men. The good news is that it is also one of the most treatable, once a man understands what is actually happening.
I am Dr Shah Dupesh, a Consultant Andrologist in Chennai. Many men assume their inability to climax with a partner means something is permanently broken. Usually nothing is broken at all — the body has simply been trained to expect a very specific kind of stimulation. Let me explain how masturbation causes this, how it differs from the medical causes that must always be ruled out, and exactly how it is reversed.
Quick Facts
- An idiosyncratic masturbation style — a very firm grip, high speed, high pressure, or rubbing against a surface — can train the body so a partner cannot reproduce the sensation needed to ejaculate.
- Prone masturbation (face-down, against a bed or floor) is the single style most often behind this.
- This is a genuine, recognised cause of delayed ejaculation, not a myth.
- The classic sign is a man who ejaculates easily alone but cannot finish during intercourse.
- Heavy pornography use and very high frequency are commonly reported to add to the problem.
- It is usually reversible: re-training the style, cutting porn, and psychosexual therapy help most men, though progress takes time.
- Delayed ejaculation also has medical causes — medications, nerve problems and hormones — that must be ruled out.
How masturbation causes delayed ejaculation
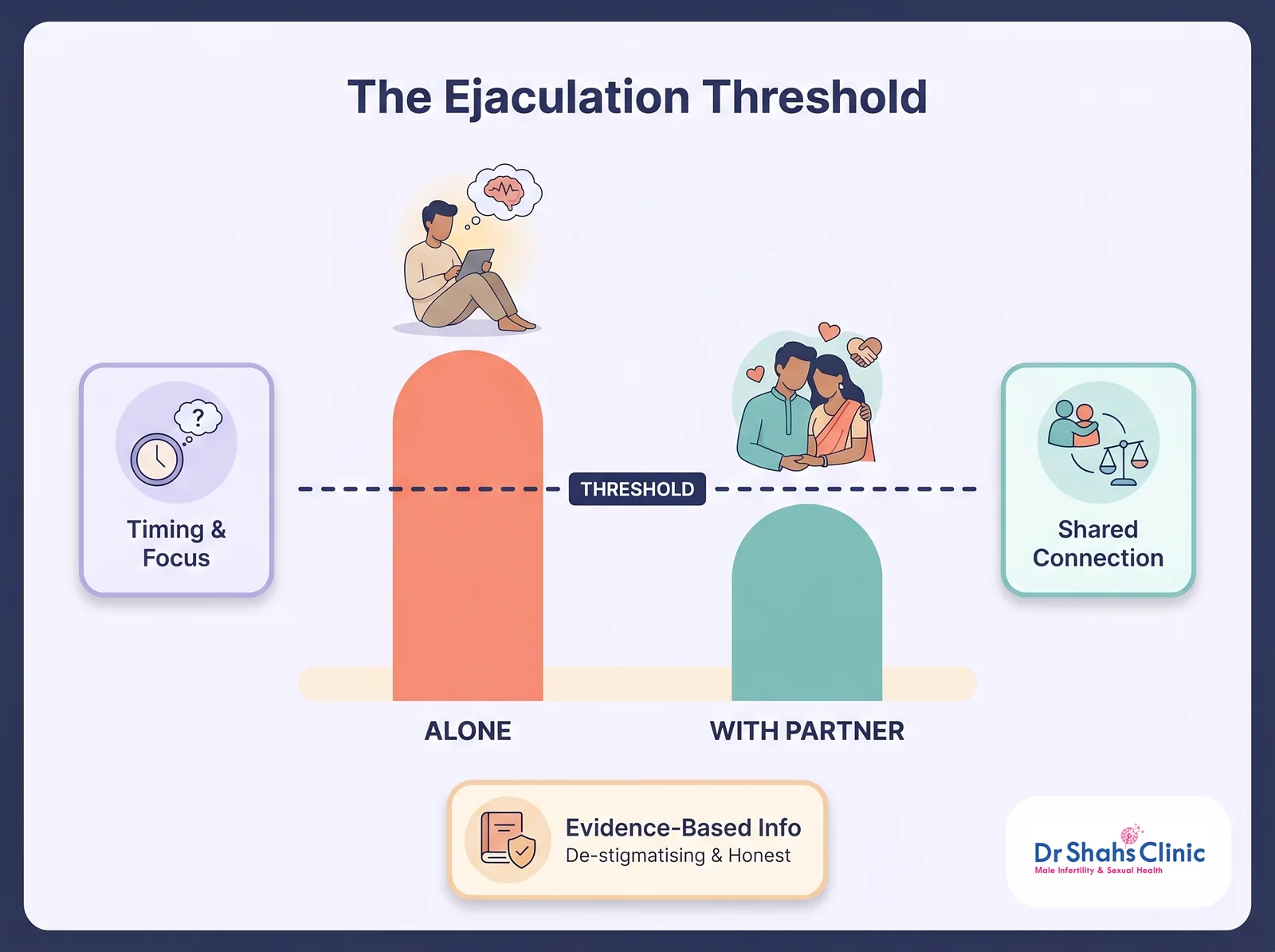
Ejaculation is a reflex with a threshold. Your body learns the level and type of stimulation that tips it over the edge, and it learns it from whatever you do most often. The problem starts when a man trains that reflex to a stimulus that real sex cannot match. Sexual-medicine specialists call this an idiosyncratic masturbation style — defined as a masturbation technique that a partner’s hand, mouth or vagina cannot easily reproduce: a grip far firmer, faster, or higher-pressure than intercourse provides, often paired with intense pornography (Perelman, 2016; Bronner & Ben-Zion, 2014).
The leading model for this is Perelman’s “Sexual Tipping Point.” Every man has a threshold at which ejaculation fires, set by a mix of physical and psychological input. Years of high-intensity, idiosyncratic masturbation push that threshold up and narrow it to one very specific kind of stimulation. When the man then has intercourse, the sensation is gentler, slower and simply different, and it never reaches the raised threshold his body now expects (Perelman, 2016). This was first described decades ago as traumatic masturbatory syndrome, and the principle still holds: the technique, not the act, is the culprit (Sank, 1998). It is worth stressing — ordinary masturbation does not do this. It is the style, the intensity, and the pairing with pornography that condition the problem.
Prone masturbation: the biggest single culprit
If there is one masturbation style most likely to cause delayed ejaculation, it is prone masturbation — lying face-down and rubbing the penis against the bed, a pillow or the floor. The pressure and friction of a firm surface are far more intense than anything a partner can provide, so the ejaculatory reflex becomes locked to a sensation that real intercourse cannot reproduce. This is no fringe observation: the original description of traumatic masturbatory syndrome was built almost entirely around prone masturbators (Sank, 1998), and prone masturbation is the style I most often find behind situational delayed ejaculation and difficulty finishing during intercourse.
It is also the hardest to undo. Unlike a tight hand grip, prone masturbation usually cannot be fixed by simply “switching technique” — recovery means stopping the prone habit completely, giving the reflex time to recalibrate, and adding proper medical treatment where needed. If you masturbate face-down, this is the single most important change you can make. We cover it in depth across these guides:
- Prone masturbation: what it is, why it harms & how to stop
- How to stop prone masturbation: a step-by-step recovery guide
- Prone masturbation: its ill effects and why to quit today
- Prone masturbation: 3 treatment strategies that work
The role of pornography
Pornography deserves its own mention, because in clinical practice it tends to compound the problem in two ways. First, the act of masturbating to porn is usually paired with the idiosyncratic grip described above, reinforcing it. Second, high-novelty, high-intensity pornographic content sets a level of visual and mental arousal that an ordinary, loving encounter rarely matches — so even when the physical technique is corrected, the arousal cue can be missing. I want to be straight about the evidence here: the published research directly linking pornography to ejaculation problems is still mixed and inconclusive. But in my clinical experience the men with the most stubborn delayed ejaculation are very often heavy, long-term porn users, and reducing it is a consistent part of their recovery. It is the same conditioning that I see driving porn-related erection problems, and the two often travel together.
What delayed ejaculation actually is
Delayed ejaculation means a marked delay in reaching climax, or being unable to climax at all, despite enough stimulation, an adequate erection and the desire to finish. In its complete form — no ejaculation at all — it is called anejaculation. It is the mirror image of premature ejaculation, and the two are the opposite ends of the ejaculatory-timing spectrum.
Doctors classify it along two lines that matter for finding the cause (Di Sante et al., 2016; Abdel-Hamid & Ali, 2018). It can be lifelong (present since a man’s first sexual experiences) or acquired (developing after a period of normal function) — and it can be generalised (happening in every situation) or situational (happening only in certain circumstances). The masturbation-style problem produces a very recognisable pattern: acquired and situational delayed ejaculation, where a man finishes easily on his own but not with a partner (Perelman, 2016). When the difficulty happens in every situation, including alone, a medical cause becomes far more likely.
It is also worth keeping a sense of proportion: delayed ejaculation is the least common of the male ejaculatory complaints, affecting roughly 1–4% of men (Chen, 2016; Di Sante et al., 2016). It is, however, deeply distressing when it happens — it strains relationships, undermines confidence, and, as we will see, can stand in the way of starting a family.
Why it happens with a partner but not alone
This situational pattern confuses men, but it is the clearest clue to the cause. Alone, a man delivers the exact high-intensity stimulation his reflex has been trained on, so he finishes easily. With a partner, the stimulation is different and gentler, and the conditioned threshold is never reached. Men with delayed ejaculation have been found to have a higher penile sensory threshold — the nerves register touch less readily — which is consistent with, though not proof of, a conditioning effect (Xia et al., 2013). The important point is that the calibration is off, not that anything is permanently damaged, and calibration can be changed.
When a man tells me he can finish in minutes on his own but cannot ejaculate inside his partner, I already have a strong idea of the cause before any test. I ask him, gently, exactly how he masturbates — the grip, the speed, the pressure, whether he lies face-down, whether porn is always involved. Almost always, the answer reveals a style no partner could ever replicate. Men are relieved to learn this, because it means they are not broken and there is a clear way back. The fix is not willpower; it is retraining — and, for the prone masturbator, the courage to stop the habit completely.
The other causes that must be ruled out
Because delayed ejaculation can also be medical, I never assume masturbation is the whole story without checking, especially when the problem happens in every situation. An honest assessment looks for the recognised medical contributors (Abdel-Hamid & Ali, 2018; Sadowski et al., 2016; Chen, 2016):
- Medications — the most common medical cause. SSRI antidepressants are the most commonly implicated; some antipsychotics, blood-pressure drugs and prostate medicines can also delay ejaculation.
- Nerve problems — diabetes is a leading culprit, as diabetic neuropathy damages the nerves that drive ejaculation; spinal cord injury and pelvic or prostate surgery can do the same.
- Hormones — low testosterone lowers sexual desire and arousal (Corona et al., 2016), and thyroid disorders are linked to ejaculatory dysfunction, classically an underactive thyroid with delayed ejaculation and an overactive thyroid with premature ejaculation (Morenas et al., 2024).
- Age — ejaculation naturally takes longer with age as penile sensitivity and nerve conduction gradually decline.
- Alcohol and recreational drugs — heavy use blunts the reflex.
- Psychological factors — performance anxiety, fear of pregnancy, guilt, depression and relationship difficulties all raise the threshold.
This is exactly why a proper evaluation matters: the treatment for a masturbation-style problem is completely different from the treatment for an SSRI side-effect, a hormone deficiency or diabetic nerve damage.
Can delayed ejaculation affect fertility?
Yes — and this is the part couples often discover too late. If a man genuinely cannot ejaculate inside the vagina, sperm never reaches the egg, so natural conception through intercourse becomes impossible even when the semen itself is perfectly healthy. Delayed ejaculation and anejaculation are therefore recognised, and very treatable, causes of difficulty conceiving. Where a couple needs to conceive and intercourse is not yet working, sperm can in selected cases be obtained using penile vibratory stimulation or electroejaculation for assisted reproduction (Sønksen & Ohl, 2002). I explain how ejaculatory problems sit within the wider fertility picture in our guide to whether masturbation causes infertility.
Talk to an andrologist about delayed ejaculation
What to expect at the consultation
Diagnosing delayed ejaculation is mostly about an honest, detailed history rather than a battery of tests (Abdel-Hamid & Ali, 2018). I ask when it started, whether it happens in every situation or only with a partner, and — the most revealing question of all — exactly how a man masturbates: grip, speed, pressure, position, and whether pornography is always involved. That single line of questioning solves the puzzle in most younger men. I also review medications (especially antidepressants), alcohol, mood, and the relationship.
A focused examination and a few targeted blood tests — testosterone, thyroid function, and blood sugar to screen for diabetes — rule out the medical causes when the pattern suggests them. There is no single “delayed ejaculation test”; the diagnosis is clinical, and the history almost always points the way.
How it is treated
When masturbation style is the cause, the treatment follows logically, though it asks for patience (Perelman, 2016; Abdel-Hamid & Ali, 2018):
- Retrain the technique. Deliberately switch to a lighter, slower grip that mimics the sensation of intercourse, so the reflex re-learns a realistic threshold. If you masturbate face-down, stop completely — see our prone masturbation recovery guide.
- Cut the pornography. High-novelty porn is widely reported to keep the arousal threshold high; reducing it lets arousal re-anchor to a real partner.
- Reduce frequency for a while, and avoid masturbating shortly before sex so you are not blunted going into intercourse.
- Psychosexual therapy, ideally involving the partner, works well — it combines the retraining above with reducing performance anxiety and rebuilding arousal around real intimacy.
- Treat any medical cause found on assessment — for example correcting a hormone problem, or reviewing a medication with the doctor who prescribed it. Never stop or change an antidepressant or any prescribed medicine on your own — that must always be done with your prescribing doctor.
It is worth being honest about the evidence: there is no drug licensed specifically for delayed ejaculation, and the formal trial base for any single treatment is limited, resting largely on case series and expert experience (Sadowski et al., 2016). What I can say from clinic is that, once the conditioning is addressed and any medical cause treated, the outlook for the masturbation-style group is genuinely good. Where the priority is conception, these techniques can often secure sperm for fertility treatment in the meantime (Sønksen & Ohl, 2002). Progress takes patience rather than a quick fix.
Book a confidential consultation
Talk to Dr Shah about delayed ejaculation, masturbation style and porn-related conditioning — discreet and judgment-free.
Free guide · no spam · unsubscribe anytime.
Myth vs Fact: masturbation and delayed ejaculation
| What you’ve been told | The clinical fact |
|---|---|
| Masturbation can never affect how you finish with a partner. | An idiosyncratic, high-intensity masturbation style — prone masturbation above all — is a recognised cause of delayed ejaculation. |
| If I can finish alone, my equipment is the problem during sex. | Finishing alone but not with a partner is the classic sign of a conditioning problem, not damage. |
| It means my nerves are permanently desensitised. | The sensory threshold is re-set high, but for the masturbation-style cause it is reversible with retraining. |
| Delayed ejaculation is always psychological. | It can be medical too — SSRIs, diabetic neuropathy, low testosterone and thyroid problems must be ruled out. |
| It has nothing to do with starting a family. | If a man cannot ejaculate inside, it directly prevents conception — but sperm can be obtained for treatment. |
| There’s nothing I can do about it. | Retraining technique, stopping prone masturbation, cutting porn and psychosexual therapy restore ejaculation in most men. |

Private 1-on-1 consultation
Can’t climax with your partner? There’s a clear reason — and a way back.
A short, private consultation identifies whether it’s masturbation style, porn conditioning, a medication or a medical cause — and gives you a real plan. No shame, no jargon.
Book a Confidential Consultation
Frequently Asked Questions
Can masturbation really cause delayed ejaculation?
Yes. An unusual or very intense masturbation style — a very firm grip, high speed, high pressure, or rubbing against a surface, often with pornography — can train the ejaculatory reflex to a stimulation a partner cannot reproduce. This is a recognised cause of delayed ejaculation, especially the kind that happens only during intercourse.
Is prone masturbation the main cause?
It is the single style I see most often behind delayed ejaculation. Masturbating face-down against a bed or floor applies a pressure and friction no partner can match, and the original description of traumatic masturbatory syndrome was based on prone masturbators. Stopping it completely — not just changing technique — is usually the key step.
Why can I ejaculate when I masturbate but not during sex?
Because alone you deliver the exact high-intensity stimulation your body has been conditioned to, while a partner provides gentler, different stimulation that never reaches that learned threshold. This situational pattern is the hallmark of a masturbation-style problem, and it is reversible.
Is the damage permanent?
When the cause is masturbation style, no — nothing is physically damaged. The sensory threshold has simply been set high by conditioning, and it can be re-set by changing your technique, stopping prone masturbation, cutting pornography, and giving the reflex time to recalibrate. (Delayed ejaculation from nerve damage or a medication is a different matter and needs medical treatment.)
Can delayed ejaculation stop me having children?
It can make natural conception difficult, because sperm has to be deposited inside the vagina. The good news is that it is treatable, and where conception cannot wait, sperm can in many cases be collected using vibratory stimulation and similar techniques for assisted reproduction.
How do I retrain my masturbation to fix delayed ejaculation?
Switch to a lighter, slower grip that mimics the sensation of intercourse rather than a tight, fast one; stop masturbating face-down entirely; cut back sharply on pornography; and reduce frequency for a while. Psychosexual therapy guides this retraining and addresses any performance anxiety.
What else causes delayed ejaculation besides masturbation?
The main medical causes are medications — especially SSRI antidepressants — diabetic nerve damage, low testosterone or thyroid disorders, ageing, heavy alcohol use, and psychological factors. A proper assessment rules these out before blaming masturbation alone.
References
- Perelman MA. Psychosexual therapy for delayed ejaculation based on the Sexual Tipping Point model. Transl Androl Urol. 2016;5(4):563-75. PMID 27652228
- Bronner G, Ben-Zion IZ. Unusual masturbatory practice as an etiological factor in the diagnosis and treatment of sexual dysfunction in young men. J Sex Med. 2014;11(7):1798-806. PMID 24674621
- Sank LI. Traumatic masturbatory syndrome. J Sex Marital Ther. 1998;24(1):37-42. PMID 9509379
- Abdel-Hamid IA, Ali OI. Delayed Ejaculation: Pathophysiology, Diagnosis, and Treatment. World J Mens Health. 2018;36(1):22-40. PMID 29299903
- Sadowski DJ, Butcher MJ, Köhler TS. A Review of Pathophysiology and Management Options for Delayed Ejaculation. Sex Med Rev. 2016;4(2):167-76. PMID 27530382
- Di Sante S, Mollaioli D, Gravina GL, et al. Epidemiology of delayed ejaculation. Transl Androl Urol. 2016;5(4):541-8. PMID 27652226
- Chen J. The pathophysiology of delayed ejaculation. Transl Androl Urol. 2016;5(4):549-62. PMID 27652227
- Xia JD, Han YF, Pan F, et al. Clinical characteristics and penile afferent neuronal function in patients with primary delayed ejaculation. Andrology. 2013;1(5):787-92. PMID 23970455
- Corona G, Isidori AM, Aversa A, et al. Endocrinologic Control of Men’s Sexual Desire and Arousal/Erection. J Sex Med. 2016;13(3):317-37. PMID 26944463
- Morenas R, Singh D, Hellstrom WJG. Thyroid disorders and male sexual dysfunction. Int J Impot Res. 2024;36(4):333-338. PMID 37752332
- Sønksen J, Ohl DA. Penile vibratory stimulation and electroejaculation in the treatment of ejaculatory dysfunction. Int J Androl. 2002;25(6):324-32. PMID 12406364
Can it be curable after quitting prone and overcome with infertility issues.
Definitely. Please quit the habit
How can I treat premature ejaculation
Levis can you please call me on 9790783856. I will do my best to help you
Definitely it can be cured