If your semen analysis report has a few values flagged in red, here’s the honest answer: one abnormal report is almost never a diagnosis. The whole art of semen analysis interpretation is reading the page line by line, against the correct reference limits — not treating it as a verdict on your fertility. Semen quality swings from week to week, and a single number on a single day rarely tells the whole story.
As a practising andrologist, I get handed these reports across my desk every single day. A man sits down, slides the paper over, and his finger is already on the one number printed in red. His face has decided the outcome before I have said a word. So let me explain what’s actually happening on that page, because once you understand how each line is measured, most of the fear quietly drains out of the room.
What a semen analysis is — and why I order it first
A semen analysis (also called a sperm test, sperm analysis or seminogram) is the single most useful first test in a man’s fertility check. It measures how much semen you produce, how many sperm it holds, how well they swim, their shape, and whether anything else — white cells, clumping, thick consistency — gets in the way.
Male factors contribute to about half of all cases when a couple struggles to conceive, and infertility touches roughly one in six couples — which is why I order a semen analysis early, alongside evaluating the partner (Katz, 2025). It is powerful — and one of the most misread documents in medicine.
Reading your semen analysis: why one red value is not a diagnosis
Here is the thing nobody tells you at the lab counter. The 2021 WHO manual (the 6th edition) deliberately swapped rigid pass-fail cut-offs for decision limits — numbers that lower the odds, not numbers that close the door. That made the test more honest, but harder to read unless you do this for a living (de Souza, 2025).
In my clinic, I see this every week: a man with one borderline result who has already convinced himself he cannot father a child. Sperm take roughly 72 to 90 days to make, so a fever, a viral illness, a stressful month or a few bad nights of sleep can all push your numbers down on test day. That is why I never act on a single report. A genuinely abnormal result gets repeated a few weeks later before it means anything at all.
Semen analysis interpretation: the reference limits that actually matter
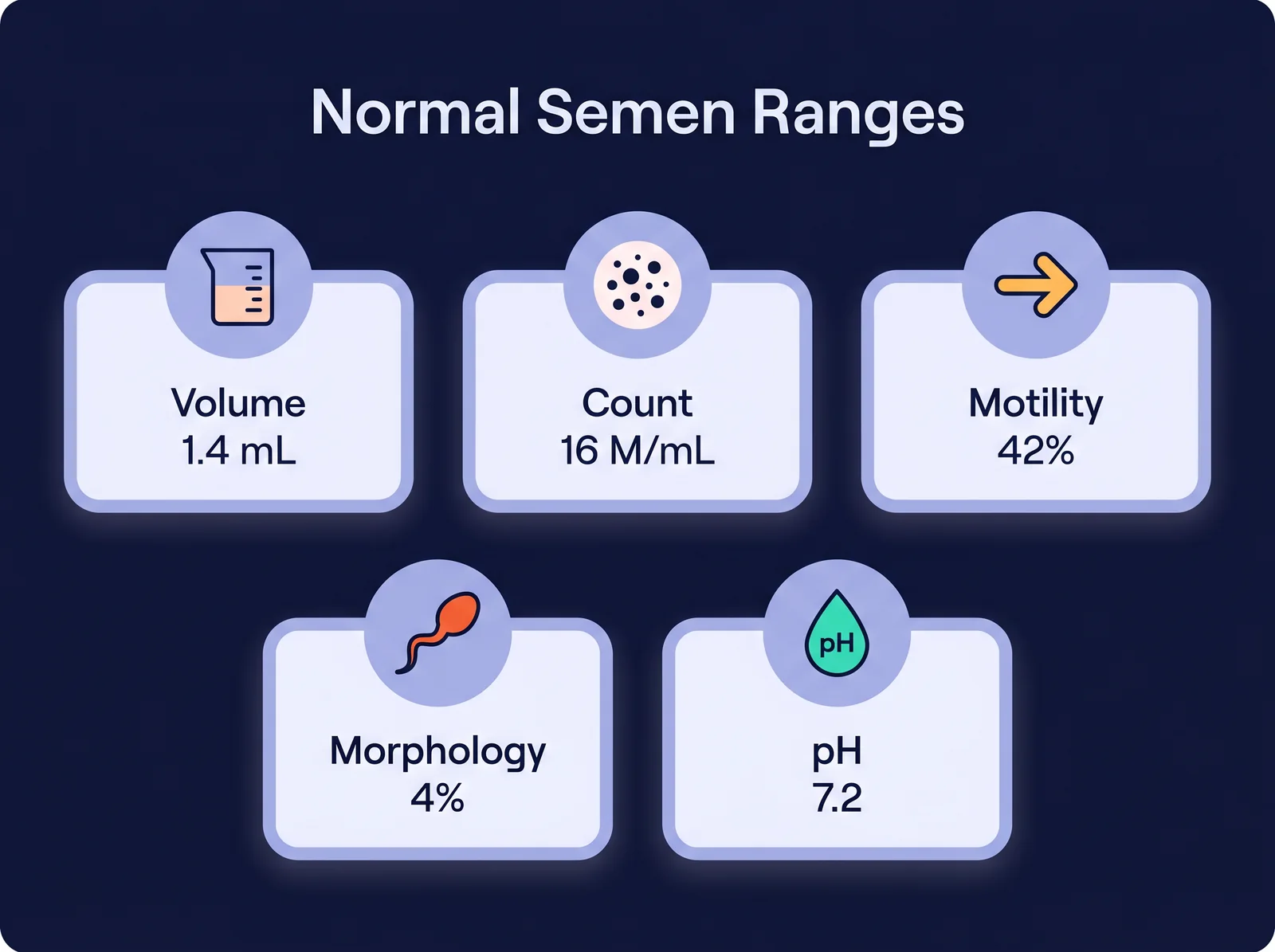
These are the lower reference limits from the 2021 WHO manual — the bottom 5th percentile of men who fathered a child within twelve months. They are the same WHO 6th-edition criteria now used to read reports worldwide (Djokoto, 2026). Read your report against these numbers, not against some imagined “perfect” score. Prefer to have it done for you? Drop your values into our free semen analysis calculator for an instant read against these WHO 2021 limits.
| Parameter | WHO 2021 lower limit | What it measures |
|---|---|---|
| Semen volume | 1.4 mL | Total fluid in the ejaculate |
| Sperm concentration | 16 million / mL | Sperm crowded into each millilitre |
| Total sperm number | 39 million / ejaculate | The headline count |
| Total motility | 42% | All sperm that move |
| Progressive motility | 30% | Sperm swimming forward |
| Vitality | 54% live | Sperm alive, moving or not |
| Normal morphology | 4% normal forms | Sperm of textbook shape |
| pH | 7.2 or above | Acid-base balance |
| Leukocytes (pus cells) | under 1 million / mL | White cells (infection signal) |
Notice how low some of these “normal” thresholds sound. That is the single most reassuring fact on the page, and almost no one explains it to you.
What your numbers mean for the time it takes to conceive
Here is the part that actually matters to a couple trying for a baby. Those WHO limits are not a fertile/infertile line in the sand — they are drawn from men whose partners conceived within twelve months. Semen quality sits on a sliding scale of time to pregnancy: the stronger your total motile count, the shorter the average time to conceive; the lower it drifts, the longer it tends to take. A recent prospective study confirmed that better semen quality tracks with higher fecundability — a faster time to pregnancy — rather than a simple yes-or-no switch (Lovett, 2025). So read a slightly low result as “this may take a little longer, and here is what we can change,” never “this is impossible.”
The names on your report: normozoospermia, oligozoospermia and the rest
Labs love long Greek words, and they frighten people more than they should — here is the plain-English glossary:
- Normozoospermia — everything is within the normal range. A clean report.
- oligozoospermia — a low sperm count (concentration or total number below the limit).
- Asthenozoospermia — low motility; the sperm are there but not swimming well.
- Teratozoospermia — a high share of abnormally shaped sperm (low morphology).
- Oligoasthenoteratozoospermia (OAT) — a mix of all three, in varying degrees.
- azoospermia — no sperm seen at all in the sample.
- Leukocytospermia (pyospermia) — too many white cells, the “pus cells” line.
Every one of these names describes one report on one day. None of them is a sentence. If you want the deeper picture on a zero count, I have written separately on azoospermia and on no sperm coming out on ejaculation.
Volume, pH and the things below the numbers
Volume is how much fluid you produced. A reading below 1.4 mL often means a short abstinence gap, anxiety on the day, or part of the sample missing the cup. Genuinely low volume that repeats — especially with a low pH — points me towards a blockage or a problem with the glands and ducts that make the fluid: fixable and identifiable, not a dead end.
pH tells a similar story. A value at or above 7.2 is what I expect; an acidic, low-volume sample is one of the few combinations that earns investigation straight away.
Below the headline numbers, your report often lists liquefaction, viscosity and appearance. Fresh semen is a gel that should liquefy within about 20 minutes; if it stays thick (high viscosity), sperm struggle to swim free, and that alone can drag the motility number down. Colour matters too — a normal sample is greyish-white, so if yours looks unusual, read my piece on green or discoloured semen and on semen that leaks out with urine rather than panicking over the main grid.
Concentration and total count: the headline number
This is the line everyone reads first. Concentration is sperm per millilitre; total count is concentration times volume. At or above 16 million per millilitre sits within range. Below the limit we call it oligozoospermia — but low does not mean zero, and modest counts achieve pregnancies every day. People ask me constantly what the normal sperm count to get pregnant is: there is no magic number — the total motile count, the forward-swimming sperm you actually deliver, guides the odds far better than concentration alone.
The genuine alarm bell is zero sperm seen, which is azoospermia and demands a proper workup — never a self-diagnosis from one slip of paper. Everything between “a bit low” and “excellent” is a spectrum I can usually push in the right direction.
Motility: forward is what counts
Motility is split into two numbers, and people routinely confuse them. Total motility (42% or above) counts every sperm that moves at all. progressive motility (30% or above) counts only the ones swimming purposefully forward — and those are the ones that matter for reaching an egg.
If total motility is good but progressive is flagged, that is useful information, not a catastrophe. Low motility — asthenozoospermia — often responds to the boring, unglamorous fixes: clearing an infection, cutting heat exposure, stopping smoking, controlling diabetes, and giving the body about three months to build a fresh batch. If motility is your problem line, I have a fuller guide on low sperm motility.
Morphology: why “4% normal” really is normal
No line on the report causes more needless panic than morphology. Patients see “4% normal forms” and read it as “96% of my sperm are broken.” That is not what it means.
Under the strict criteria we use today, even men with proven fertility — men whose partners conceived naturally within the year — averaged only around 9.98% normal forms in a reference study of fertile men (Fu, 2025). Fewer than one in ten sperm look textbook-perfect in fertile men. The 4% threshold was never a grade out of a hundred — it is a deliberately low decision limit.
On top of that, morphology is the least reproducible measurement in the test — the same slide read in two labs can give two different percentages, which is why expert groups now advise against over-reading morphology defects (Gatimel, 2025). If morphology is your only flagged value, it is often the least worrying line on the page.
Vitality, pus cells and agglutination: the lines people skip
Vitality (54% live or above) matters most when motility is very low — it tells me whether still sperm are dead or simply lazy, and the two need different solutions. Plenty of live-but-immobile sperm points to a structural tail problem, not a dead sample.
Leukocytes are white blood cells — the line your report may call pus cells. The normal range is under one million per millilitre. Above that (leukocytospermia), I investigate for inflammation or infection — a raised count flags further testing rather than confirming infection by itself, and higher seminal white-cell counts have been linked to greater sperm DNA fragmentation (Peng, 2026) — more on what pus cells in semen mean. Agglutination — sperm clumping — can hint at an immune (antibody) factor. None of these is a death sentence; each is a clue to a specific, treatable cause.
What your semen analysis report does not tell you
Here is what I always say in the consulting room: a normal semen analysis is reassuring, but it is not a fertility certificate, and an abnormal one is not a sentence. What it cannot show is why — and the most valuable next step is almost always the sperm-production hormones, not an exotic add-on.
You will have heard of sperm DNA fragmentation — breaks in the genetic material inside the head, which a routine analysis cannot see. It is real: high fragmentation tracks with lower concentration, motility and vitality (Ejehi, 2026), and everyday factors feed in, such as low vitamin D (Marisamy, 2026). But let me be very clear, because the testing industry will not tell you this: a DNA fragmentation (DFI) test is not a routine investigation. Its routine use is genuinely contested (Pandiyan, 2017), and in twelve years of practice I can count on one hand the number of times I have ordered it — reserved for the rare couple with recurrent miscarriage or repeated failed treatment cycles. For almost everyone else it adds cost and anxiety, not answers.
The test I actually reach for is a hormone profile. FSH, LH and testosterone are the engine-room readouts of sperm production — markers of both how many sperm you make and how well you make them — and they often tell me more than an isolated semen analysis ever could. A low testosterone, FSH or LH is not bad news; it is frequently the most fixable finding on the table, because the right hormonal medication can correct it and lift sperm production in a way no supplement can. This is exactly why a global standard now folds proper male evaluation into every stage of the fertility pathway, rather than stopping at one semen report (Esteves, 2026).
What actually causes an abnormal semen analysis
When a report comes back low, the cause is usually one of a familiar, addressable handful: an untreated infection; heavy smoking, alcohol or drugs; obesity and uncontrolled diabetes; long heat exposure from laptops, saunas or hot workplaces; certain medicines; and plain age. Studies applying the WHO 6th-edition criteria keep finding lifestyle factors sitting squarely among the commonest contributors to abnormal semen parameters (Djokoto, 2026). The reason this matters for interpretation is simple: an abnormal line is a question — “why?” — not a full stop.
Can you improve your semen analysis results?
Often, yes — and this is where I spend the most time reassuring men. Because sperm regenerate on that 72-to-90-day cycle, the right move after an abnormal report is to fix the underlying cause and clean up the modifiable factors, then retest in about three months. Stop smoking, lose excess weight, treat the infection, cool the testes, control the diabetes. And where the hormone profile is off, the right hormonal medication to correct a low testosterone, FSH or LH can restore sperm production at its source — a real, targeted fix, not a guess in a bottle.
What I steer men away from — firmly — is the shelf of antioxidant “fertility booster” pills: CoQ10, L-carnitine, L-arginine and the rest. Let me be blunt: they do not work, and a supplement industry profits handsomely from selling men hope in a bottle. This is not just my opinion — a large randomised trial (the MOXI study) found antioxidants did not improve semen parameters or live-birth rates in infertile men (Steiner, 2020), and the Cochrane review finds only low-certainty evidence of any benefit, with signals of possible harm to live births (de Ligny, 2022). So skip the bottles. Chase the cause, give it a full sperm cycle, and judge by the repeat test — not by the marketing on a label.
A word on home and online semen tests
Mail-order and pharmacy “fertility kits” are everywhere now, and patients ask me about them constantly. They have a role for a rough, private first look — but a recent review found these direct-to-consumer products vary widely in what they measure and how closely they follow clinical standards (Ernandez, 2025). A kit that checks only concentration can hand you a comfortable green tick while quietly missing motility, morphology and every other line we have just walked through. Treat them as a doorbell, not a diagnosis.

Private 1-on-1 consultation
Want your report read, line by line?
Bring your semen analysis in and I will interpret every line with you — what is normal, what is not, and exactly what to do next.
Book a Confidential Consultation
How to give the test its best shot
A little preparation makes the result far more honest. The WHO manual suggests two to seven days of abstinence, but here is where I part company with the textbook: I ask my patients for just one day. When I analysed more than two thousand semen reports across different abstinence periods, longer abstinence did not improve the sample — it tends to drag motility down — while a short gap of around a day gives a truer, often better result (Dupesh, 2020). So the men who “save up” for a fortnight usually hand me a worse report, not a better one. Collect the whole sample (the first, sperm-rich portion is most often lost), keep it warm, and get it to the lab within the hour. Skip the test during or just after a fever, and tell the lab about any medication you take.
And then repeat it. A diagnosis on any abnormal parameter needs at least two samples, usually a few weeks apart, before it means anything. I have lost count of the men whose “terrible” first report turned completely normal on the second, once a fever or a brutal month at work had passed. That is the single most important rule of semen analysis interpretation: never let one bad day on paper become your diagnosis.
When to see a specialist about your semen analysis
Book a proper review if a repeat report stays abnormal, shows azoospermia or raised pus cells, or if you have been trying for a year (six months if your partner is over 35). Then I add what the basic report cannot give: a hormone profile, a clinical examination, sperm DNA fragmentation, and genetic tests when the count is very low — the staged evaluation one report was never meant to replace.
Quick Facts
- The WHO 2021 lower limit for sperm concentration is 16 million/mL — and “low” is not “zero.”
- Even proven-fertile men average only about 9.98% normal sperm morphology (Fu, 2025).
- Sperm regenerate on a 72-to-90-day cycle, so an abnormal report must be repeated.
- Progressive motility (30%+) matters more than total motility for natural conception.
- The normal range for pus cells (leukocytes) is under 1 million/mL.
- The sperm-production hormones (FSH, LH, testosterone) should be checked — they reflect both the quantity and quality of sperm production and often tell us more than an isolated semen analysis.
Get this as a printable guide
Prefer to keep it? Call the clinic and we will send you this complete semen-analysis guide as a PDF you can read anytime.
Frequently Asked Questions
How do I read my semen analysis report?
Compare each value to the 2021 WHO lower limits — concentration 16 million/mL, total motility 42%, progressive 30%, morphology 4%, volume 1.4 mL — and treat any single flagged value as a reason to repeat the test, not a diagnosis. These are decision limits, not pass-fail marks (de Souza, 2025).
What is a normal semen analysis report?
One where every parameter is at or above the WHO 2021 limits — volume 1.4 mL, concentration 16 million/mL, total sperm 39 million, total motility 42%, progressive 30%, vitality 54%, morphology 4%, pH 7.2, pus cells under 1 million/mL. An all-normal report is called normozoospermia.
What do oligozoospermia, asthenozoospermia and teratozoospermia mean?
Low count, low motility, and a high share of abnormally shaped sperm, respectively; azoospermia means no sperm at all. Each describes one report, not your destiny.
What does pus cells in semen mean, and what is the normal range?
Pus cells are white blood cells; the normal range is under 1 million per millilitre. A raised result (often reported as “8–10 pus cells”) prompts a check for inflammation or infection — it flags testing, not a confirmed infection.
Is 70% sperm motility normal?
Yes, comfortably — the WHO limits are 42% total and 30% progressive motility, so 70% is well within range as long as a good share is progressive, forward-swimming movement.
Is 2.5 mL sperm volume normal?
Yes — the lower limit is just 1.4 mL. Volume matters most when very low and paired with a low pH, which can suggest a blockage.
Is 7% normal sperm morphology good?
Yes — it is above the 4% threshold, and even fertile men average under 10% normal forms (Fu, 2025), so 7% is reassuring.
What is a normal sperm count to get pregnant?
A concentration at or above 16 million/mL with at least 39 million total sits in the fertile range; lower counts still conceive, and the total motile count matters more than one number.
Can a normal semen analysis still miss a fertility problem?
Yes — it does not look inside the sperm, so it can miss high DNA fragmentation, worth testing after recurrent miscarriage or failed cycles (Ejehi, 2026).
Can I improve my semen analysis results?
Often, yes — treat the cause and fix lifestyle over about three months and the repeat test improves; antioxidant pills are not the answer (Steiner, 2020).
Get your report read properly
A semen analysis is a map, not a sentence — and good semen analysis interpretation means reading every line in context, against the right limits. If your report worries you, bring it in and let us read it together, alongside the rest of your history.
Book a Consultation — andrologycorner.com/contact/ · +91 97907 83856
References
- Esteves SC (2026). The WHO 2025 Guideline for the Prevention, Diagnosis and Treatment of Infertility: A Comprehensive Review with Focus on Male Reproductive Health. International braz j urol : official journal of the Brazilian Society of Urology. PMID 41770990
- Katz DJ, O’Donnell L, McLachlan RI, Moss TJ, Boothroyd CV, Jayadev V, Catford SR (2025). The first Australian evidence-based guidelines on male infertility. The Medical journal of Australia. PMID 41208521
- Gatimel N, Barbotin AL, Mery L, Beauvillard D, Bendayan M, Boursier A, Boueilh T, Pereira B, Chammas J, Jacquet JC, Levy R, Pfeffer J, Pons-Rejraji H, Sanguinet P, Brugnon F (2025). Recommendations for Human Sperm Morphology Assessment in 2025: An Expert Review From the French BLEFCO Group. Andrology. PMID 41185394
- Fu L, Zhou F, Chen G, Yuan R, Li W, Qiu S, Tang L, Liu W, Gu Y, Lu W (2025). Morphological Parameters of 29994 sperm in a fertile male population-based on Papanicolaou staining and SSA-II Plus. Frontiers in endocrinology. PMID 40123889
- de Souza GL, Lozano AFQ, Hallak J (2025). SPG360° and SpermoMAP: a functional and stratified interpretation model for human semen analysis in frontline fertility care. European journal of obstetrics, gynecology, and reproductive biology. PMID 41240874
- Ejehi MA, Mirfakhraie R, Tavalaee M, Naderi N, Izadi T, Nasr-Esfahani MH (2026). Inflammasome-related markers and long non-coding rnas in seminal plasma: Associations with sperm DNA fragmentation and male infertility. Journal of reproductive immunology. PMID 42128473
- Peng L, Wang T, Zhu M, Le Y, Yang S (2026). Association of semen leukocytes with sperm DNA fragmentation in a clinical cohort. Frontiers in endocrinology. PMID 42255418
- Ernandez J, Cook G, Berk B, Berger AJ, Kathrins M (2025). Direct-to-consumer semen analysis products: Content, accountability, and adherence to clinical guidelines. Andrology. PMID 39806828
- Djokoto RMK, Owusu VB, Agana EA, Nduroh KA, Arthur-Komeh J, Adarkwa O, Vormawor AP, Ofori AA, Adu IK (2026). Lifestyle factors and prevalence of semen abnormalities among men undergoing infertility evaluation at oak specialist hospital: A retrospective cohort study. PloS one. PMID 41538375
- Marisamy P, Jayapal P, Mageswaran R, Krishnan Selvaraj M, Arthanari K (2026). Serum 25-Hydroxyvitamin D and Sperm DNA Fragmentation Index In Men Referred For Infertility: A Cross-Sectional Study of 783 Patients. Journal of family & reproductive health. PMID 42088472
- Steiner AZ, Hansen KR, Barnhart KT, Cedars MI, Legro RS, Diamond MP, Krawetz SA, Usadi R, Baker VL, Coward RM, Huang H, Wild R, Masson P, Smith JF, Santoro N, Eisenberg E, Zhang H (2020). The effect of antioxidants on male factor infertility: the Males, Antioxidants, and Infertility (MOXI) randomized clinical trial. Fertility and sterility. PMID 32111479
- de Ligny W, Smits RM, Mackenzie-Proctor R, Jordan V, Fleischer K, de Bruin JP, Showell MG (2022). Antioxidants for male subfertility. The Cochrane database of systematic reviews. PMID 35506389
- Lovett SM, Sommer GJ, Krivorotko D, Wesselink AK, Rothman KJ, Hatch EE, Eisenberg ML, Wise LA (2025). A prospective study of semen quality and fecundability among North American couples planning pregnancy. Andrology. PMID 40646671
- Dupesh S, Pandiyan N, Pandiyan R, Kartheeswaran J, Prakash B (2020). Ejaculatory abstinence in semen analysis: does it make any sense? Therapeutic advances in reproductive health. PMID 32596668
- Pandiyan N, Pandiyan R, Raja DR (2017). A perspective on sperm DNA fragmentation. Translational andrology and urology. PMID 29082196
Visit us in Chennai
A private, judgment-free space to talk through fertility and men’s sexual health. Walk in, or book ahead by phone.
📍No 21, Sree Kalki Apartments, Ground Floor, Bazullah Road, T-Nagar, Chennai 600017